Pancreatic Ductal Adenocarcinoma
By: Thelonius Chang, Dublin High School


The Effect of Mutated SMAD4 genes on the TGF-ß pathway
The SMAD4 gene comes from the SMAD family of genes that interacts with the TGF-ß pathway in the cell. The absence of SMAD4 is commonly found within Pancreatic Ductal Adenocarcinoma (PDAC) cells, and is associated with decreased rate of survival for patients suffering from the condition. The SMAD4 gene contains 12 exons and 11 introns throughout the entire sequence, and is located on the 18th chromosome on arm q band 21.2 (18p21.2). combined with the TGF-ß pathway, and acting as a major component of the pathway for signal transduction can both help suppress and promote tumor growth in different circumstances. Other than PDAC, absence of SMAD4 is found in Myhre's Syndrome and various other forms of cancer.

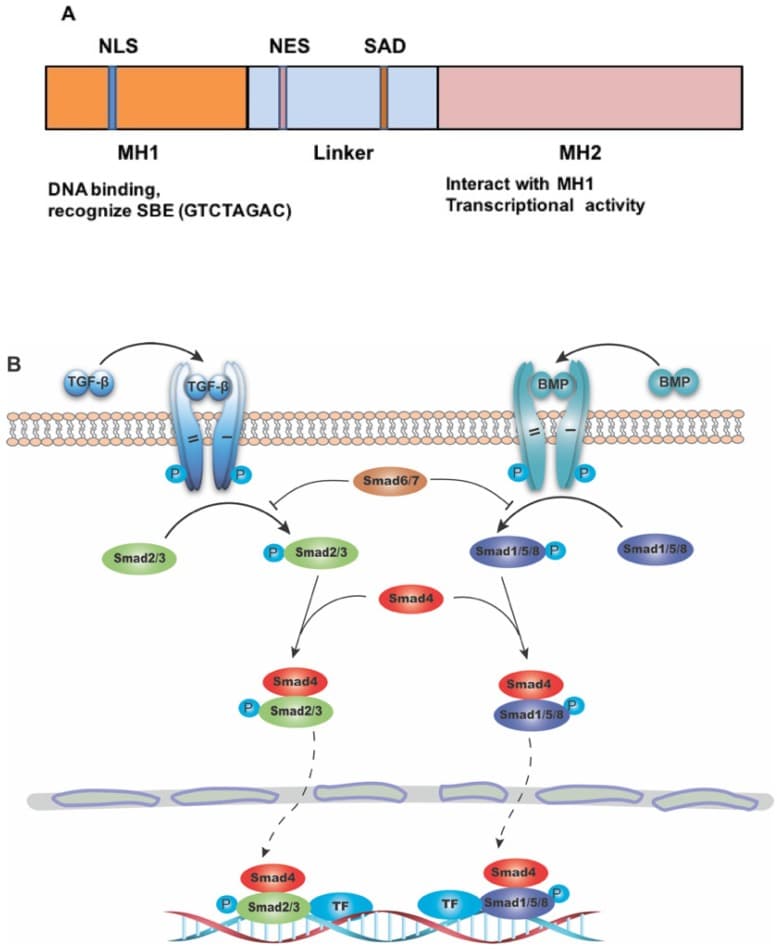
The structure of SMAD4 and its role as the common mediator for signaling of TGF-β superfamily. (source)
What is Pancreatic Ductal Adenocarcinoma (PDA)?
It is a type of pancreatic cancer that is very common among pancreatic cancer patients. It begins in the exocrine compartment of the pancreas. WIthin the tumor the most important cells include cancer-associated fibroblasts and pancreatic stellate cells, which help create an extracellular matrix barrier against medicine. Certain immune cells like regulatory T-cells or macrophages can also limit other CD8+T cells from performing the task of targeting cancer cells, of which are often recruited to the tumor site.
The cancer itself is very lethal, having an extremely low survival rate as a result of failure for traditional cancer therapy treatments such as chemotherapy, surgery, and radiation to address the tumor. One of the most effective treatments against early stage PDAC is surgery combined with chemotherapy; however, PDAC is very difficult to catch early since symptoms do not show until it has developed to later stages. Therefore, the treatment can only be applied to lucky patients that have been diagnosed early, before the tumor has had time to metastasize and develop the extracellular matrix. In addition to this, mutations in genes like KRAS or SMAD4 have shown to increase resistance to therapy due to affecting cellular pathways.
Mechanism
SMAD4 plays a significant role in the TGF-ß pathway and signal transduction in which activated receptors can start the formation of SMAD2/3 complexes which are completed with the addition of SMAD4. After this, the complex can connect with other transcription factors in the nucleus to perform suppression or transcription work on genes. Members of the SMAD family utilize a ß-hairpin loop on the N-terminal Mad Homology Domain 1 (MH1) to connect to and physically interact with the DNA while using an α-Helix-2 domain on MH2 for interaction with transcriptional factors. SMAD assemblies specifically attach to SMAD Binding Elements, which use variations of GTCT and AGAC nucleotides.


Transforming growth factor β (TGF-β) signaling pathway plays important roles in many biological processes, including cell growth, differentiation, apoptosis, migration. (source)
Some of these genes help regulate the presence of tumors and can help initiate apoptosis in case of irreversible cell damage at G1 or S checkpoints. Depending on the transcription factor they attach to, they can express genes that perform apoptosis themselves or can begin the caspase cascade through cytochrome C promotion. As a result, a mutation preventing the presence of SMAD4 can lead to a pro-tumor environment that is apoptosis resistant and has the ability to metastasize more easily. SMAD4 also helps prevent TGF-ß's limiting of the PTEN tumor suppressor, which without can lead to a more aggressive cancer. Other ways the presence of SMAD4 limits tumor growth or the absence promotes tumor growth can been seen with p21, a protein that helps induce apoptosis which can be increased with the help of SMAD4.
Although the loss of SMAD4 is significant in resulting in increase maliciousness of cancers, due to the many roles the TGF-ß pathway plays throughout the cellular system, it can also benefit patients in certain circumstances. For example, the TGF-ß and SMAD4 interaction can lead to Epithelial-mesenchymal Transition (EMT), a process in which specialized cells become more stem-like and have increased mobility, making them more capable of spread through metastasis. This is especially dangerous if cancer is able to undergo EMT and spread. In fact, the TGF-ß pathway, although initially having the ability to restrict tumors, can in later stages play the role of supporting its progression through this phenomenon. Of course, even though the TGF-ß pathway may be hindered in later stages, EMT can still occur as it can still stem from many other pathways. One thing to note is that although impaired SMAD4 can be associated with PDAC, it has not been shown that a SMAD4 mutation can actively start cancer. Lack of SMAD4 can only decrease the rate of survival of patients, while usually the cancer is initiated with mutations of other genes such as Kras.
Basic Model of the TGF-ß Pathway with SMAD4
Once the TGF-ß ligand binds to the receptors, the TGF-ß receptors 1 and 2 combine and use the SARA protein to connect SMAD2 and 3 into one structure. This structure then connects with SMAD4 so that it can begin expressing proteins in the nucleus. Once in the nucleus, it needs to bind to a transcriptional factor in order to start expressing genes. As shown in the model, TGF-ß results in both tumor restrictive and tumor supportive (in later stages of PDAC) effects. Without SMAD4, TGF-ß would not be able to access this tumor suppressing pathway, thus leading to the proliferation of cancer such as PDAC.

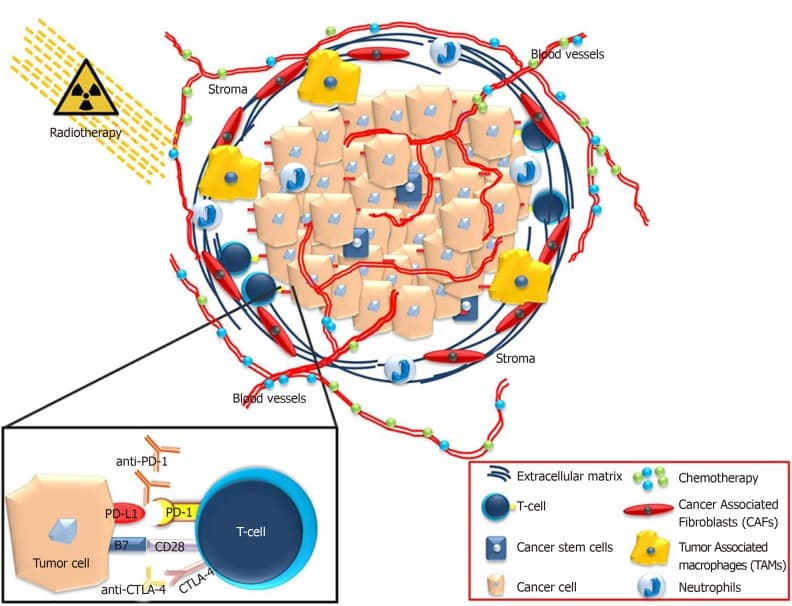
Τhe pancreatic ductal adenocarcinoma microenvironment consists of a significant hurdle for the efficient application of chemotherapy drugs or immunotherapeutic compounds. (source)
Discussion & Future direction:
PDAC has a major effect on much of the cancer patient population, due to its high death rate and low chance of survival over a long period of time. This is because PDAC works in a way in which traditional treatments to cancer are near ineffective—especially due to the thick extracellular matrix that can help prevent treatments from reaching the cancer effectively. Understanding how PDAC works, associated mutations, and possible treatments can have a huge impact on these cancer patients, turning what seems like a hopeless prognosis into the potential to wipe out the cancer. Although reintroducing the previously mentioned SMAD4 protein into cells to help reverse the progression of cancer isn't too effective, new developments in general approaches to cancer bring the possibility for new treatment. Immunotherapy is one such new treatment that has been promising for a number of different cancers people tend to face. It works by trying to trigger an immune response to have the immune system wipe out the cancerous cells.
Immunotherapy itself did not work well on PDAC cells, but research is now directed towards immunotherapy combined with other traditional methods, such as chemotherapy. The aggressiveness of PDAC comes from its heterogeneity. It is a type of cancer that stems from various different mutations in the genome, meaning that not one single treatment is going to work well against it. As a result, the new combined therapy approach, with immunotherapy and others, is a very promising solution for the future. What matters most for a cancer like this is finding out what works against cells with specific mutations, then mixing together methods tailored to fighting each differing PDAC cell. There is also the idea of cancer stem cells in PDAC, which help increase the chances of the cancer coming back. Therapy specifically made to counter these stem cells along with all the other heterogeneous members of the tumor may be significant when it comes to PDAC treatment research.
_ By: Thelonius Chang, Dublin High School _ (External student, guest post on the request of Mentors)
References
- https://www.phosphosite.org/proteinAction.action?id=1845&showAllSites=true
- https://www.ncbi.nlm.nih.gov/gene/4089
- https://pubmed.ncbi.nlm.nih.gov/29483830/
- https://omim.org/entry/139210
- https://reactome.org/PathwayBrowser/#/R-HSA-170834
- https://pubmed.ncbi.nlm.nih.gov/33008426/
- http://www.indianjcancer.com/article.asp?issn=0019-509X;year=2011;volume=48;issue=3;spage=351;epage=360;aulast=Singh
- https://www.ijbs.com/v14p0111.htm
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7031151/
The opinions expressed here are the views of the writer and do not necessarily reflect the views and opinions of Elio Academy.