Coronary Heart Disease
Understanding the contributing factors to coronary heart disease and how do they manifest.

By: Almari Rheeder, Beijing City International School
Introduction
Coronary heart disease is a disease in which fatty deposits made up of cholesterol and other cellular materials (plaque) accumulate inside the coronary arteries on the surface of the heart, leading to the narrowing of the arteries." (World Health Organization) It is the most common heart disease in the United States of America.
Causes
Prolonged tobacco use has a strong correlation with diagnosis of coronary heart disease. This includes smoking and secondhand smoke from tobacco and tobacco products such as vape and cigarettes. High cholesterol, diabetes/insulin resistance, high blood pressure, not getting enough exercise and smoking or tobacco use may be the causes of damage to the coronary arteries.

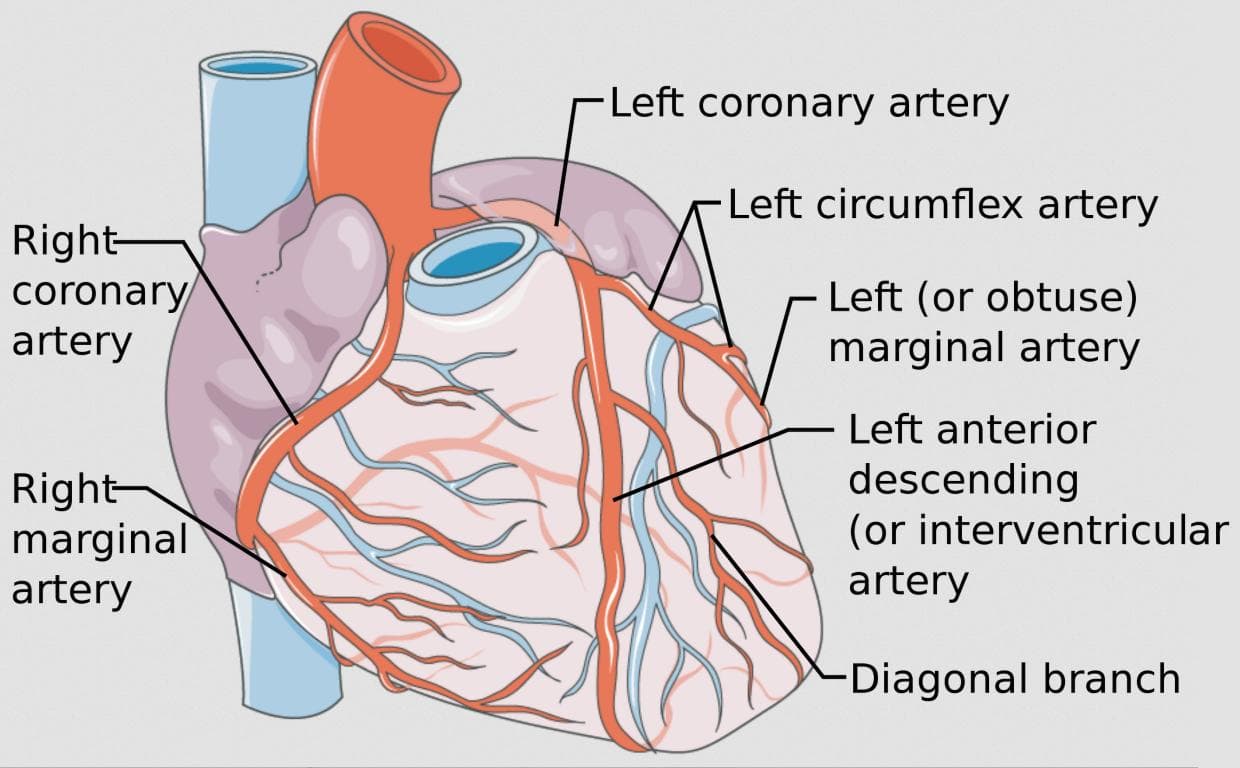
Healthy coronary arteries (Source)
Risk factors
There are several risk factors that are associated with increasing the likelihood of CHD. Some of the well known risk factors are:
- Age: as you get older, risk of damaged or tightened arteries increases
- Sex: Men are typically at a higher risk of coronary artery disease. For women, the risk increases after they reach menopause
- Family history: Risk is highest if your father or brother had heart disease before the age of 55 or if your mother or sister developed it before the age of 65
- Smoking: People who smoke have a significantly higher risk of heart disease
- High blood pressure: Uncontrolled high blood pressure can increase the risk of the coronary arteries becoming narrow, which slows blood flow
- High cholesterol: Bad cholesterol is called low-density lipoprotein cholesterol. Not enough good cholesterol also leads to atherosclerosis (a disease of the arteries characterized by the deposition of fatty material on their inner walls)
- Diabetes: Type 2 diabetes and CHD share some risk factors
- Obesity: Can lead to type 2 diabetes and high blood pressure
- Chronic kidney disease: long term increases risk
- Not enough exercise: Sedentary lifestyle is linked to CHD
- Lots of stress: Emotional stress may damage the arteries and worsen risk factors
- Unhealthy diet: Eating foods with lots of saturated fat, trans fat, salt and sugar can increase risk
- Alcohol use: Heavy alcohol usage can lead to heart muscle damage
- Amount of sleep: Too little and too much sleep, have both been linked to an increased risk of heart disease
Prevention
CHD can be prevented up to certain extent by strategies and actions to promote healthy lifestyle and reduce the likelihood of the disease. Some approaches could :
- No/quit smoking
- Control high blood pressure, high cholesterol, and diabetes
- Exercise often
- Maintain a healthy weight
- Eat a low-fat, low-salt diet that's rich in fruits, vegetables, and whole grains
- Reduce and manage stress
Symptoms
CHD can manifest with a range of symptoms that vary in intensity and presentation. Some of the common symptoms include-
- Angina (chest pain): a condition marked by severe pain in the chest, often also spreading to the shoulders, arms, and neck, owing to an inadequate blood supply to the heart
- Fatigue: extreme tiredness resulting from mental or physical exertion or illness
- Decrease in work productivity: workers tend to loose motivation
- Shortness of breath: struggle to breathe
- Heart attack: women may have less typical symptoms such as neck or jaw pain, nausea and fatigue. Some heart attacks don't cause any noticeable symptoms
- Heart failure: heart doesn't pump blood as it should
- Arrhythmias** :** not enough blood to the heart can alter normal heart signalling, leading to irregular heart
Cite: https://www.sujyotheartclinic.com/symptom-of-heart-disease-in-adults/

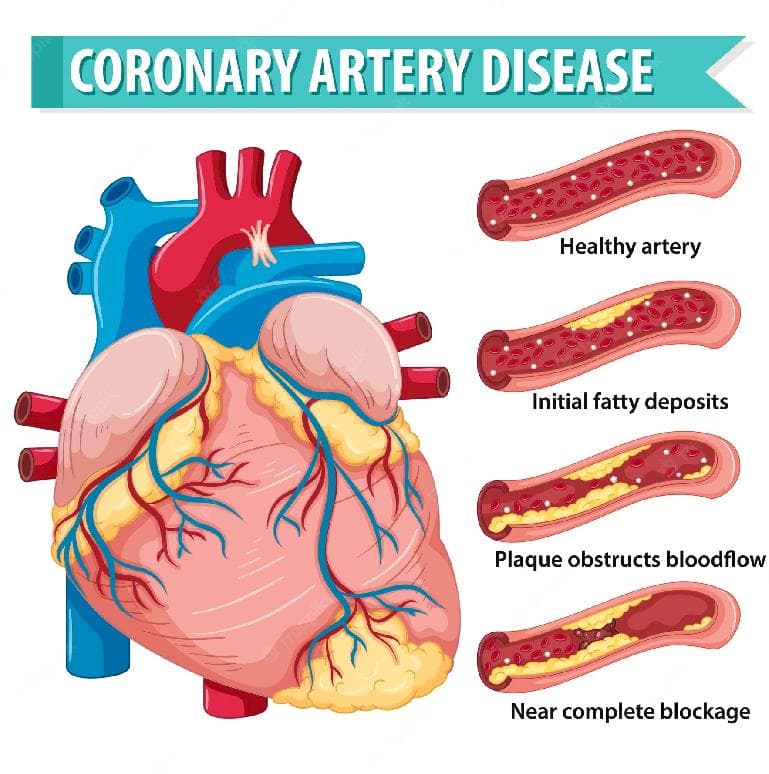
Plaque buildup in the coronary arteries (Source)
Diagnosis methods
Several diagnostic methods are used to assess CHD. These methods help healthcare professionals evaluate the extent of blockages or narrowing in the coronary arteries and determine appropriate treatment. Common diagnostic techniques include:
- Electrocardiogram (ECG or EKG): Can show how fast or slow the heart is beating
- Echocardiogram: Uses sound waves to create pictures of the beating heart
- Exercise stress test: Walk on a treadmill or ride a stationary bike during an ECG
- Nuclear stress test: Shows how blood moves to the heart muscle at rest and during stress
- Heart (cardiac) CT scan: Show calcium deposits and blockages in the heart arteries
- Cardiac catheterization and angiogram: Insert flexible tube (catheter) into a blood vessel, usually in the wrist or groin. Outlines any blockages.
Mechanism of Action
A decreased flow to the heart of blood containing oxygen, which may result in a heart attack and could cause serious harm to the heart or abrupt death. Typically, this happens slowly over a long period of time, and many individuals with this condition are only made aware after they suffer from a severe heart attack.
Molecular insight
According to Chu et al., the levels of pentraxin 3 protein were higher in subjects with coronary artery disease compared to those in the control group. However, it's important to note that correlation does not imply causation. Therefore, there isn't a definitive link to support the notion that the PTX3 protein directly contributes to the development of coronary artery disease.

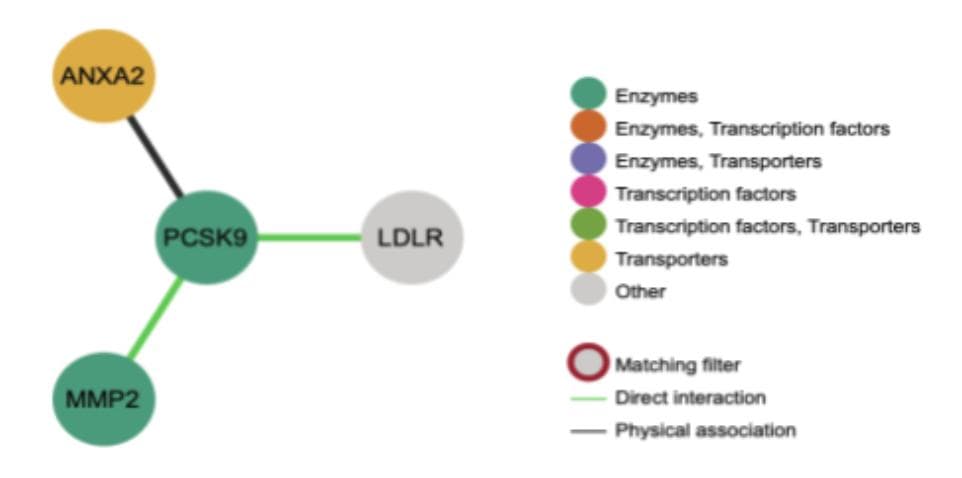
PCSK9's interactions with other proteins in the body (Source)
Certain proteins have been identified as potentially related to coronary artery disease. One such protein is Apolipoprotein A5 (APOA5), which plays a crucial role in regulating plasma triglyceride levels in the blood—a recognized risk factor for coronary artery disease. APOA5 is a component of high-density lipoprotein (HDL), also known as 'good' cholesterol, responsible for cholesterol absorption and transport to the liver. Mutations in this gene can lead to elevated triglyceride levels, potentially contributing to coronary artery disease. A study published in the Journal of Lipid Research highlighted a connection between APOA5 gene mutations and hypertriglyceridemia—a condition marked by high fat concentrations in the blood, associated with various cardiovascular diseases, including coronary heart disease. This gene is situated on chromosome 11 and consists of 118 amino acids.
Another protein implicated in coronary heart disease is Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9), which plays a pivotal role in regulating plasma cholesterol homeostasis—a state of equilibrium among interdependent elements, maintained by physiological processes. Imbalanced cholesterol levels resulting from disrupted homeostasis can contribute to coronary artery disease. The molecular functions of this gene encompass hydrolase and protease activities, and its expression occurs in kidney, liver, and intestine tissues. PCSK9 facilitates the transport of specific receptors responsible for lysosome degradation and influences fatty acid and cholesterol metabolism. Autosomal dominant familial hypercholesterolemia, characterized by elevated cholesterol levels in the bloodstream, has been associated with PCSK9 gene mutations.

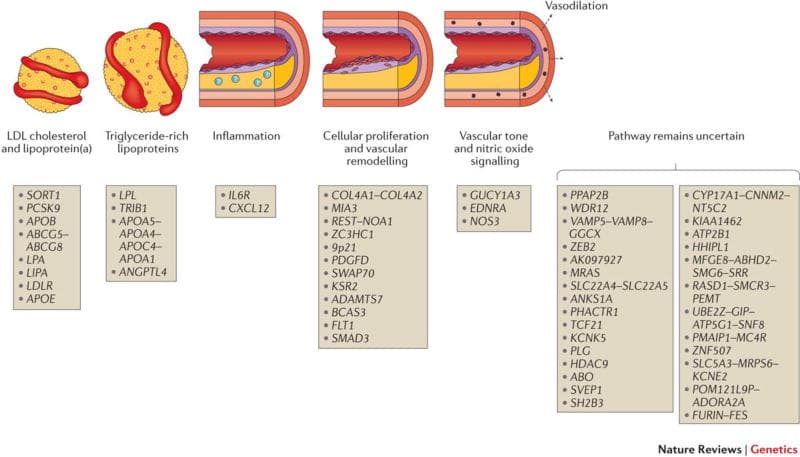
Illustration of the influence of various proteins on the coronary arteries (Source)
Notably, this gene interacts with three distinct proteins: ANXA2, MMP2, and LDLR. Among these interactions, direct associations exist with MMP2 and LDLR. ANXA2, a protein coding gene, enhances tumor development, invasion, and metastasis. MMP2, a protein, contributes to the regulation of inflammatory signaling cascades. The LDLR gene encodes the low-density lipoprotein receptor, the primary transporter of cholesterol in the blood. These interactions provide evidence supporting the link to coronary heart disease—since inflammation in coronary arteries is a contributor to coronary artery disease, and elevated blood cholesterol levels lead to plaque accumulation, obstructing blood flow to the heart.
Treatment and Clinical management
Individualized treatment plans are based on the severity of CHD, the presence of other medical conditions, and the patient's overall health. Regular communication with healthcare providers and adherence to recommended treatments are key to effective clinical management and improved outcomes for individuals with CHD.
Medications
- Cholesterol drugs
- Aspirin
- Beta blockers
- Calcium channel blockers
- Angiotensin-converting enzyme
Conclusion
The APOA5 and PCSK9 genes are associated with coronary heart disease and may act as contributing factors to the inflammation and constriction of coronary arteries when mutations in these genes are present. These mutations can be hereditary, potentially leading to future cardiovascular health issues. Individuals with close genetic ties to affected individuals are at a higher risk of developing coronary heart disease. To prevent the onset of this condition, adopting a healthy lifestyle is essential. This includes maintaining a balanced diet, engaging in regular exercise, managing stress, refraining from smoking, and moderating alcohol intake to promote cardiovascular well-being.

Click to view enlarged poster.

Click to read full paper.
Impact Statement

Hello! My name is Almari Rheeder and I am an 18 year old from South Africa, but currently in my senior year of high school in Beijing, China. My project is about CHD (coronary heart disease) and how it manifests. I investigated the causes, risk factors, prevention, and molecular insight regarding this disease. During this course, I learned a lot about genetics, genomics, and their importance for study in the medical fields. This program has opened me up to making new friends in other places in the world, and has inspired me to consider a wider range of careers within the medical field.
Student Reflection
Work cited (APA)
- Chu, Y., Teng, J., Feng, P., Liu, H., Wang, F., & Li, X. (2019). Pentraxin-3 in coronary artery disease: A meta-analysis. Cytokine, 119, 197–201. https://doi.org/10.1016/j.cyto.2019.03.017
- Hilfiker-Kleiner, D., Landmesser, U., Drexler, H. (2006). Molecular Mechanisms in Heart Failure: Focus on Cardiac Hypertrophy, Inflammation, Angiogenesis, and Apoptosis.Critical Issues in Cardiovascular Research, 48(9), A56-A66.https://www.sciencedirect.com/science/article/pii/S0735109706018080
- Jansen, H., Samani, N. J., & Schunkert, H. (2014). Mendelian randomization studies incoronary artery disease. European heart journal, 35(29), 1917–1924. https://doi.org/10.1093/eurheartj/ehu208
- Khera, A. V., & Kathiresan, S. (2017). Genetics of coronary artery disease: discovery, biology and clinical translation. Nature reviews. Genetics, 18(6), 331–344. https://doi.org/10.1038/nrg.2016.160
- Korzonek-Szlacheta, I., Danikiewicz, A., Szkodziński, J., Nowak, J., Lekston, A., Gąsior, M.,Zubelewicz-Szkodzińska, B., & Hudzik, B. (2018). Relationship Between Plasma Pentraxin 3 Concentration and Platelet Indices in Patients With Stable Coronary Artery Disease. Angiology, 69(3), 264–269.https://doi.org/10.1177/0003319717732929
- Mayo Clinic Staff. (2022, May 25). Coronary Artery Disease. Mayo Clinic. Retrieved August 1, 2023, from www.mayoclinic.org/diseases-conditions/coronary-artery-disease/symptoms-causes/syc-20350613.
- Suzuki, S., & Takeishi, Y. (2018). Molecular mechanisms and clinical features of heart failure. Fukushima journal of medical science, 64(3), 116–124.https://doi.org/10.5387/fms.2018-17
Project done at Elio Academy of Biomedical Sciences
By: Almari Rheeder
The opinions expressed here are the views of the writer and do not necessarily reflect the views and opinions of Elio Academy.