Acute Myeloid Leukemia
Understanding the Relation to FLT3 Mutations

By: Chance White, Saint Ignatius College Preparatory
Introduction
Acute Myeloid Leukemia (AML) is an aggressive cancer of the blood and bone marrow which inhibits normal hematological development. The disease is characterized by abnormal proliferation of premature white blood cells known as myeloid cells. The uncontrolled colonial expansion of myeloid cells inhibits erythropoiesis (healthy red blood cell division) in patients and can result in a subsequent plethora of malicious illnesses including bone marrow failure. Normally, blood stem cells process their development first forming myeloids, then myeloblast stage, and finally white blood cells.

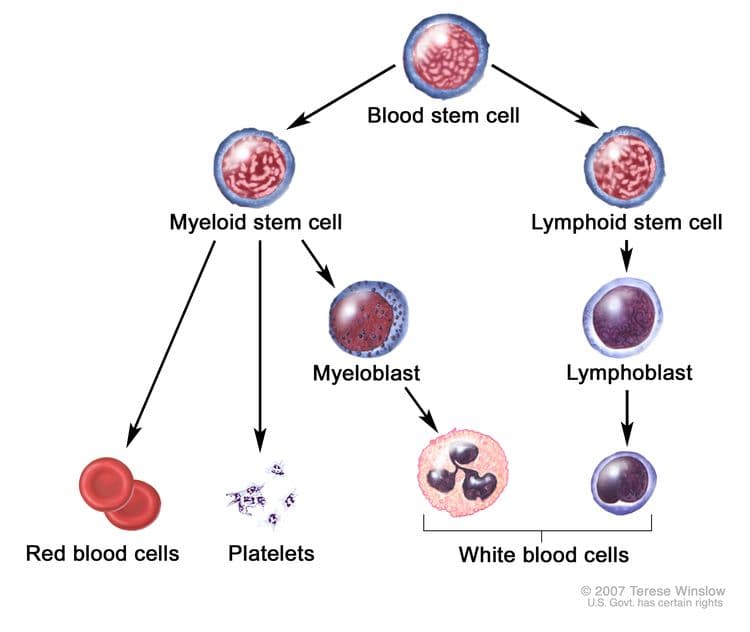
Diagram exhibits the stages of blood cell development, starting from a blood stem cell (Source)
The most prevalent cause of this disease is a mutation in the FLT3 gene, with approximately 30% of all AML cases stemming from an FLT3 mutation. This gene is one which creates and regulates the Tyrosine Kinase Receptors (RTKs) of myeloid cells. RTKs inhabit the cell surface and typically initiate healthy cell division. In healthy cases, these receptors are created in normal quantitative amounts, and must pair up to form dimers before activation. However, these receptors, once mutated, are no longer constrained by dimers nor quantity apexes, and thus overexpress and uncontrollably cue cell proliferation. In mutated cases, RTKs cue the premature white blood cell to divide too much, and the patient is left with an unhealthy amount of myeloid cells, which, in excess, are known as myeloblasts, or "blasts" for short. Naturally, blasts take up too much space in patients bone marrow and blood, and subsequent problems arrive.
Disease information
Acute Myeloid Leukemia typically presents itself in symptoms such as pale or "washed out" skin, tiredness, breathlessness, unprompted weight loss, frequent infections, fever, and unusual and frequent bleeding (such as bleeding gums or nosebleeds), although asymptomatic cases are not uncommon.
Possible tests for an AML diagnosis include
Complete blood counts:
In most cases of suspected AML, complete blood counts (CBCs) are performed to determine the cellular makeup of a patient's blood and bone marrow. Any number of myeloblasts greater than a 2:10 ratio (20%) is deemed cancerous, with a 1:20 ratio (5%) deemed healthy.
Bone marrow aspirates and biopsies:
When AML is suspected, doctors might extract bone marrow from patients and perform biopsies to determine if cancer is present. A bone marrow extraction is called an aspirate, and the subsequent analysis is called a biopsy
DNA sequencing:
In more specific cases, when the patient is suspected to have mutation-based AML, DNA sequencing can be performed to confirm the specific mutation causing the disorder.
Immunophenotyping by flow cytometry:
In cases where immunophenotyping is used, scientists look at sick patients' cells under a microscope to better determine the specific disease contracted. For AML, scientists look for irregularities, such as specific antigens on the cell surface.

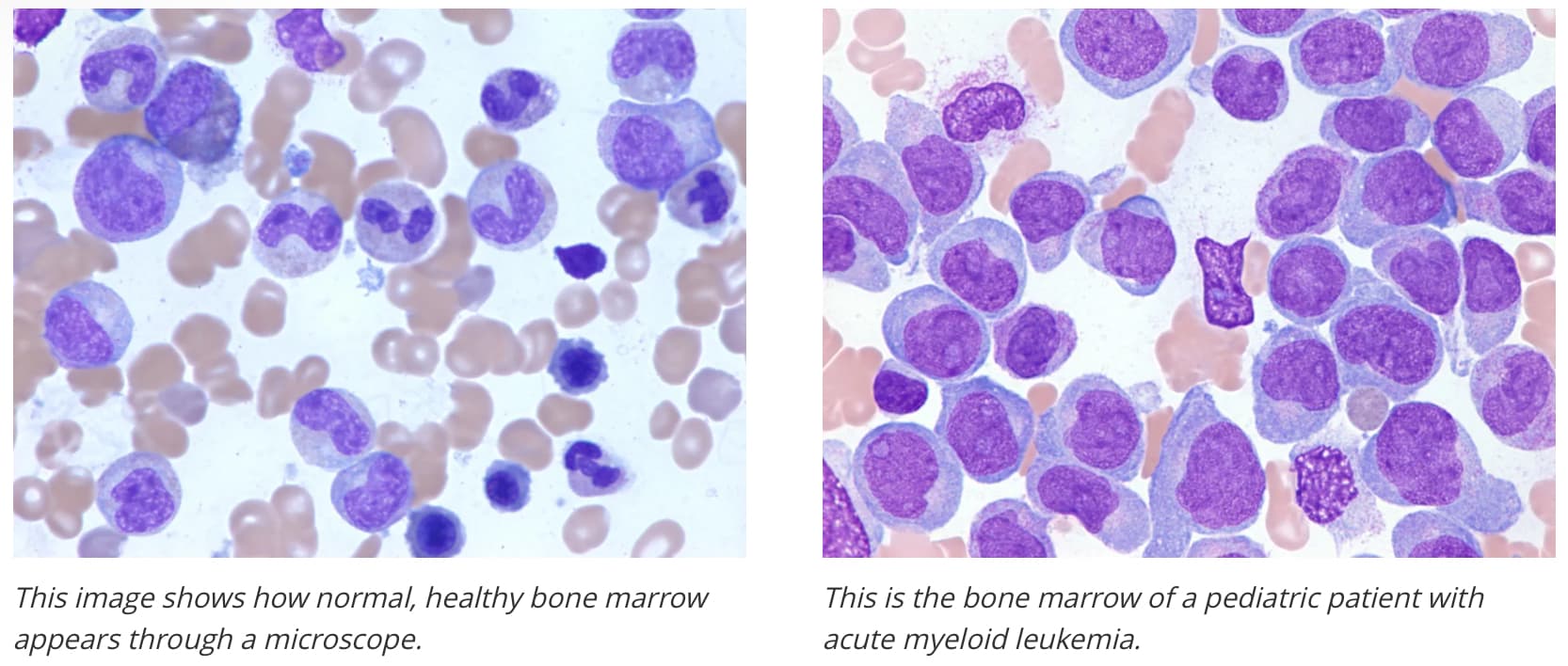
Side by side comparison of bone marrow, comparing healthy to AML positive, left to right, respectfully. (Source)
Current available treatment for AML includes
Chemotherapy:
As with most cancers, when a patient is diagnosed with AML, doctors might prescribe drugs that target rapidly dividing cells. These drugs are known as chemotherapy.
Radiation therapy:
Radiation therapy is typically prescribed with a diagnosis of cancer, and is designed to target dangerous cells. In AML cases, doctors might prescribe radiation therapy with the hope of targeting blasts.
Bone marrow transplant:
In cases of AML, patients often exhibit unhealthy blood ratios within their veins and bone marrow. To combat this, doctors often use bone marrow transplants to provide the patient with healthy ratios from an outside source.
Targeted drug therapy (FLT3 inhibitors):
In some cases of AML, monoclonal antibodies, or cancer targeting antigens, such as in the drug Gemtuzumab ozogamicin are used to attack the cancerous blasts. These antigens attach to the cancerous myeloblasts and initiate apoptosis within the cancerous cells.
However, in cases of AML in which the patient has a mutation in the FLT3 gene, Type I tyrosine kinase inhibitors (TKIs) such as midostaurin and gilteritinib or type II FLT3 inhibitors such as quizartinib are used. Type I TKIs bind the FLT3 receptor in the active conformation, either near the activation loop or the ATP-binding pocket, and are active against ITD and TKD mutations. Conversely, Type II TKIs bind the FLT3 receptor in the inactive conformation in a region adjacent to the ATP-binding domain, and are active against specifically ITD mutations. Overall, these drugs block RTKs from receiving the proliferation signals and thus decrease overall cell multiplication.

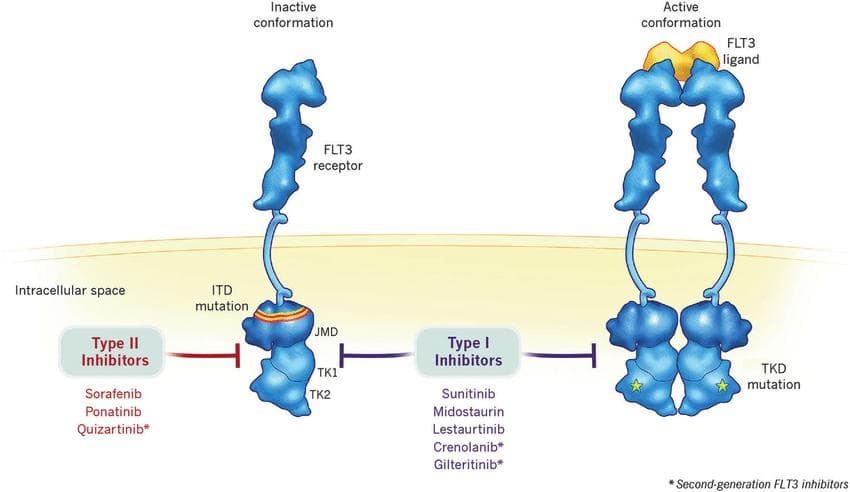
A visual demonstration of Type I and Type II FLT3 inhibitors, such as midostaurin or gliternib and quizartinib, respectively. (Source)
Gene level information
The majority of Acute Myeloid Leukemia cases are caused by variations in the FLT3 gene, a gene responsible for the creation and regulation of the Tyrosine Kinase Receptors (TKRs), which are located on the cell's surface. In AML, approximately 30% of cases have FLT3 mutations. These mutations come in two main types: internal tandem duplications (ITD) in the juxtamembrane domain (23% of cases) and point mutations in the tyrosine kinase domain (TKD) (7% of cases).
In contrast, the FLT3-TKD mutation does not significantly affect outcomes in AML. Therefore, many studies investigating FLT3 inhibitors have focused on patients with FLT3-ITD mutations.

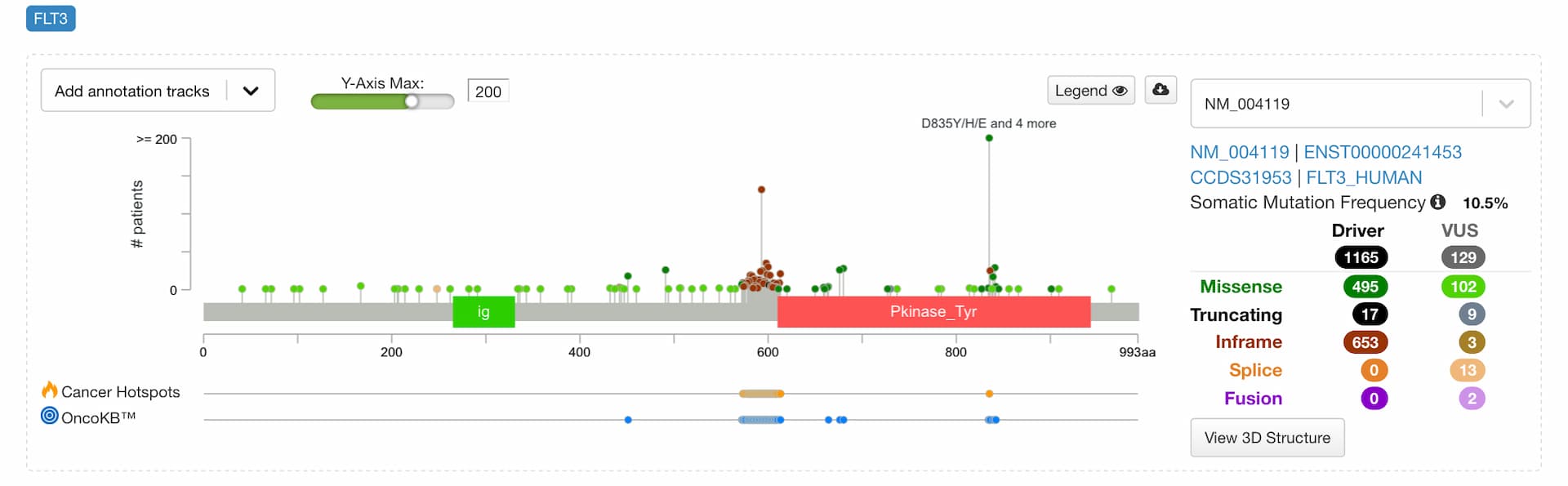
Graph by CBioPortal exhibits recorded mutations in the FLT3 gene; 1294 Mutations: includes 195 duplicate mutations in patients with multiple samples (Source)
Research
Routine cancer care is rapidly evolving to include tyrosine kinase inhibitors (TKIs). RTKs have been proven to be at root of several cancers including AML, and thus, a drug which tackles the prevention of the misexpression of RTKs is desperately needed. In regards to AML, extensive research has come forth presenting the most recently approved TKI, quizartinib.

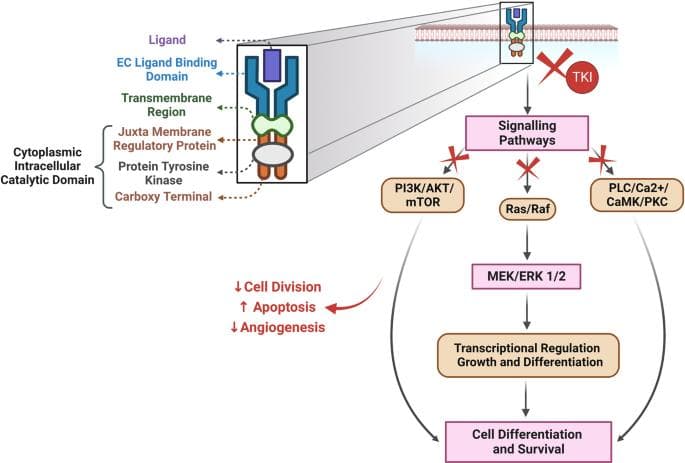
Illustration explains FLT3 receptors and how TKIs inhibit the adverse effects of mutations. (Source)
Quizartinib, a drug designed specifically to target cancerous cells in patients with diagnosed FLT3-ITD AML, has been extensively researched in regard to its effect on RTKs; Quizartinib is designed to selectively inhibit FLT3 mutations . To do this, quizartinib routinely blocks RTKs from receiving the tyrosine kinase the normally would, thereby preventing the RTK from cueing unnecessary cell proliferation.
A recent clinical trial (QuANTUM-First (NCT02668653)) concluded that "Quizartinib is a potent inhibitor of FLT3 autophosphorylation in wild-type and ITD-mutated FLT3 cells."

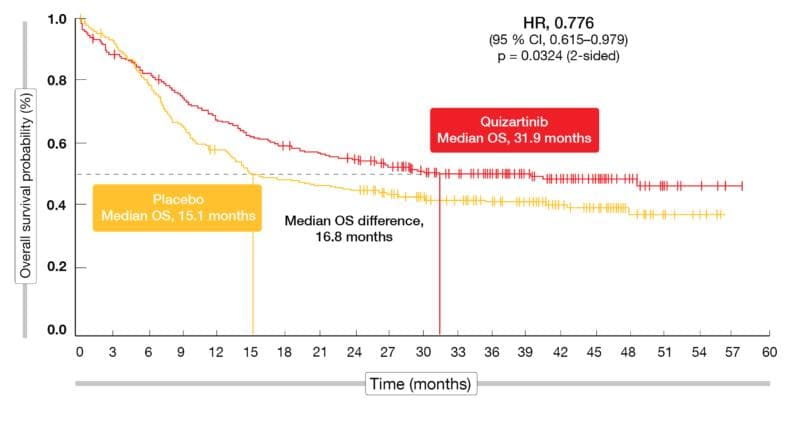
Overall survival probability in patients with FLT3-ITD mutations is superior upon the addition of quizartinib in the QuANTUM-First trial. (Source)
The FDA approved Quizartinib for use in FLT3-ITD AML positive patients on July 20, 2023.
Future directions of research
Next set of experiments
Since the early 2000s, TKIs have been used to treat various cancers including hematological malignancies such as AML. However, TKIs can lead to harmful effects on the body. Several TKIs have been linked to cardiovascular issues (high blood pressure, irregular heartbeat, and heart failure), but each drug has its own adverse side effects. Quizartinib, for example, has been linked to several bodily disorders including Neutropenia and Thrombocytopenia. We don't fully understand why these effects occur, which makes treatment and guidelines uncertain.
In terms of future directions of research and development, the adverse side effects of TKI drugs should be examined and prevented. New studies should be implemented with the purpose of designing a more helpful drug with less severe side effects. More can be learned about the specific effects of each TKI, and better preventative measures can be determined in future studies.
Furthermore, as DNA sequencing becomes readily available to everyday patients, individualized medicine becomes more prevalent across the medical field. With regards to AML, this DNA sequencing could supply an easier diagnosis to doctors, and help them choose the correct treatment path. In the future, sequencing will likely become easier, and thus, so will AML treatment.
Conclusion
AML is a dangerous and aggressive cancer that needs to be combated, whether pharmaceutically or otherwise. Although recent developments in TKIs such as the invention of quizartinib and other pharmaceuticals, have come forth, these drugs cause adverse effects which may be detrimental to patients overall health. As of 2023, there is no definite, perfect way to diagnose and treat AML, or any disease, for that matter.
That being said, the medical field evolves everyday, and I look forward to witnessing the personalized medical field that will more accurately target and treat disease in the near future. With pharmaceutical development evolving, I look forward to the more personalized drugs of the future, and the better, safer treatment of diseases such as AML.

Click to view enlarged poster.

Click to read full paper.
Impact Statement

My name is Chance White, and for my research project at Elio Academy, I chose to research Acute Myeloid Leukemia. In the report, I delve into the specific gene mutations which cause this disorder, choosing specifically to focus on mutations in the FLT3 gene, a gene which is responsible for the creation and regulation of Tyrosine Kinase Receptors. I choose this topic because my grandfather was recently diagnosed with a similar sickness, and I want to better understand his situation and treatment options. Overall, my time at the Elio Academy was highly informative and engaging. I learned about genes and genetics in great detail, and now understand a great deal more about the functions and limits of our wide genomes. I would recommend this program to anyone pursuing a career in medicine, or anyone who is simply interested in learning more about the biology of the world around us.
Student Reflection
References
- Kiyoi, Hitoshi, et al. "FLT3 Mutations in Acute Myeloid Leukemia: Therapeutic Paradigm beyond Inhibitor Development." Cancer Science, vol. 111, no. 2, Feb. 2020, pp. 312–22. PubMed Central, https://doi.org/10.1111/cas.14274
- "Leukemia - Symptoms and Causes." Mayo Clinic, https://www.mayoclinic.org/diseases-conditions/leukemia/symptoms-causes/syc-20374373
- Acute Myeloid Leukemia Treatment - NCI. 7 June 2023, https://www.cancer.gov/types/leukemia/patient/adult-aml-treatment-pdq
- Gilliand, D. Gary and Griffin, James D. "The roles of FLT3 in hematopoiesis and leukemia." American Society of Hematology. 1 Sep. 2002. https://ashpublications.org/blood/article/100/5/1532/106333/The-roles-of-FLT3-in-hematopoiesis-and-leukemia
- Du, Zhenfang, and Christine M. Lovly. "Mechanisms of Receptor Tyrosine Kinase Activation in Cancer." Molecular Cancer, vol. 17, no. 1, Feb. 2018, p. 58. BioMed Central, https://doi.org/10.1186/s12943-018-0782-4
- FLT3 Fms Related Receptor Tyrosine Kinase 3 [Homo Sapiens (Human)] - Gene - NCBI. https://www.ncbi.nlm.nih.gov/gene/2322
- Leukemia (Blood Cancer) : Symptoms, Signs, Causes, Types & Treatment Made Easy. www.youtube.com, https://www.youtube.com/watch?v=orzNVoFv7K8
- Inc, Mechanisms in Medicine. "Treating AML." You and AML, https://www.YouAndAML.com/en-aml/view/m401-a04-treating-aml-animation
- "Acute Myeloid Leukemia (AML)." Cleveland Clinic, https://my.clevelandclinic.org/health/diseases/6212-acute-myeloid-leukemia-aml
- Daver, Naval, et al. "Targeting FLT3 Mutations in AML: Review of Current Knowledge and Evidence." Leukemia, vol. 33, no. 2, 2019, pp. 299–312. PubMed Central, https://doi.org/10.1038/s41375-018-0357-9
- "Targeting FLT3 Mutations in AML: Review of Current Knowledge and Evidence." Leukemia, vol. 33, no. 2, Feb. 2019, pp. 299–312. www.nature.com, https://doi.org/10.1038/s41375-018-0357-9
- Du, Zhenfang, and Christine M. Lovly. "Mechanisms of Receptor Tyrosine Kinase Activation in Cancer." Molecular Cancer, vol. 17, no. 1, Feb. 2018, p. 58. BioMed Central, https://doi.org/10.1186/s12943-018-0782-4
- Grafone, Tiziana, et al. "An Overview on the Role of FLT3-Tyrosine Kinase Receptor in Acute Myeloid Leukemia: Biology and Treatment." Oncology Reviews, vol. 6, no. 1, Apr. 2012, p. e8. PubMed Central, https://doi.org/10.4081/oncol.2012.e8
- Kampa-Schittenhelm, Kerstin Maria, et al. "Quizartinib (AC220) Is a Potent Second Generation Class III Tyrosine Kinase Inhibitor That Displays a Distinct Inhibition Profile against Mutant-FLT3, -PDGFRA and -KIT Isoforms." Molecular Cancer, vol. 12, Mar. 2013, p. 19. PubMed, https://doi.org/10.1186/1476-4598-12-19
- Mongre, Raj Kumar, et al. "Emerging Importance of Tyrosine Kinase Inhibitors against Cancer: Quo Vadis to Cure?" International Journal of Molecular Sciences, vol. 22, no. 21, Oct. 2021, p. 11659. PubMed Central, https://doi.org/10.3390/ijms222111659
- Quizartinib With Standard of Care Chemotherapy and as Continuation Therapy in Patients With Newly Diagnosed FLT3-ITD (+) Acute Myeloid Leukemia (AML) - Full Text View - ClinicalTrials.Gov. https://clinicaltrials.gov/ct2/show/NCT02668653
- Receptor Tyrosine Kinases (Newer Version). www.youtube.com, https://www.youtube.com/watch?v=-osiUGKsu7o
- Research, Center for Drug Evaluation and. "FDA Approves Quizartinib for Newly Diagnosed Acute Myeloid Leukemia." FDA, July 2023. www.fda.gov, https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-quizartinib-newly-diagnosed-acute-myeloid-leukemia
- Shyam Sunder, Sunitha, et al. "Adverse Effects of Tyrosine Kinase Inhibitors in Cancer Therapy: Pathophysiology, Mechanisms and Clinical Management." Signal Transduction and Targeted Therapy, vol. 8, no. 1, July 2023, pp. 1–27. www.nature.com, https://doi.org/10.1038/s41392-023-01469-6
- "Adverse Effects of Tyrosine Kinase Inhibitors in Cancer Therapy: Pathophysiology, Mechanisms and Clinical Management." Signal Transduction and Targeted Therapy, vol. 8, no. 1, July 2023, pp. 1–27. www.nature.com, https://doi.org/10.1038/s41392-023-01469-6
- Tests for Acute Myeloid Leukemia (AML). https://www.cancer.org/cancer/types/acute-myeloid-leukemia/detection-diagnosis-staging/how-diagnosed.html
- Thomson, Robert J., et al. "Tyrosine Kinase Inhibitors." StatPearls, StatPearls Publishing, 2023. PubMed, http://www.ncbi.nlm.nih.gov/books/NBK563322/
- What's New in Acute Myeloid Leukemia (AML) Research? https://www.cancer.org/cancer/types/acute-myeloid-leukemia/about/new-research.html
- Yamaoka, Toshimitsu, et al. "Receptor Tyrosine Kinase-Targeted Cancer Therapy." International Journal of Molecular Sciences, vol. 19, no. 11, Nov. 2018, p. 3491. PubMed Central, https://doi.org/10.3390/ijms19113491
- Zhou, Fang, et al. "Quizartinib (AC220): A Promising Option for Acute Myeloid Leukemia." Drug Design, Development and Therapy, vol. 13, 2019, pp. 1117–25. PubMed, https://doi.org/10.2147/DDDT.S198950
Project done at Elio Academy of Biomedical Sciences
By: Chance White
The opinions expressed here are the views of the writer and do not necessarily reflect the views and opinions of Elio Academy.