Sweat Allergy
By: MinJi Seo, Harbin Wanbang School

Introduction
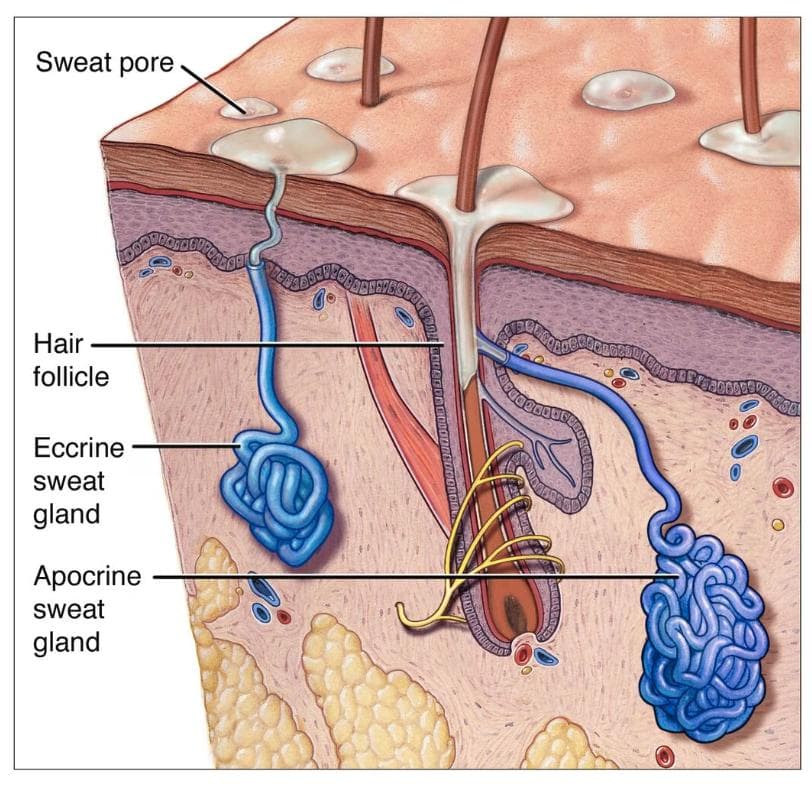
Sweating is a vital bodily function for temperature regulation. When body temperature rises, the hypothalamus signals eccrine sweat glands to release water, cooling the body. These glands excrete a liquid mixture containing water, sodium, potassium, amino acids, and more. This fluid, known as sweat, aids temperature reduction through evaporative cooling. However, certain individuals react allergically to a sweat component named MGL_1304, causing skin redness and itching. This condition, termed sweat allergy, is a type I hypersensitivity reaction against sweat constituents.
What is Sweat Allergy

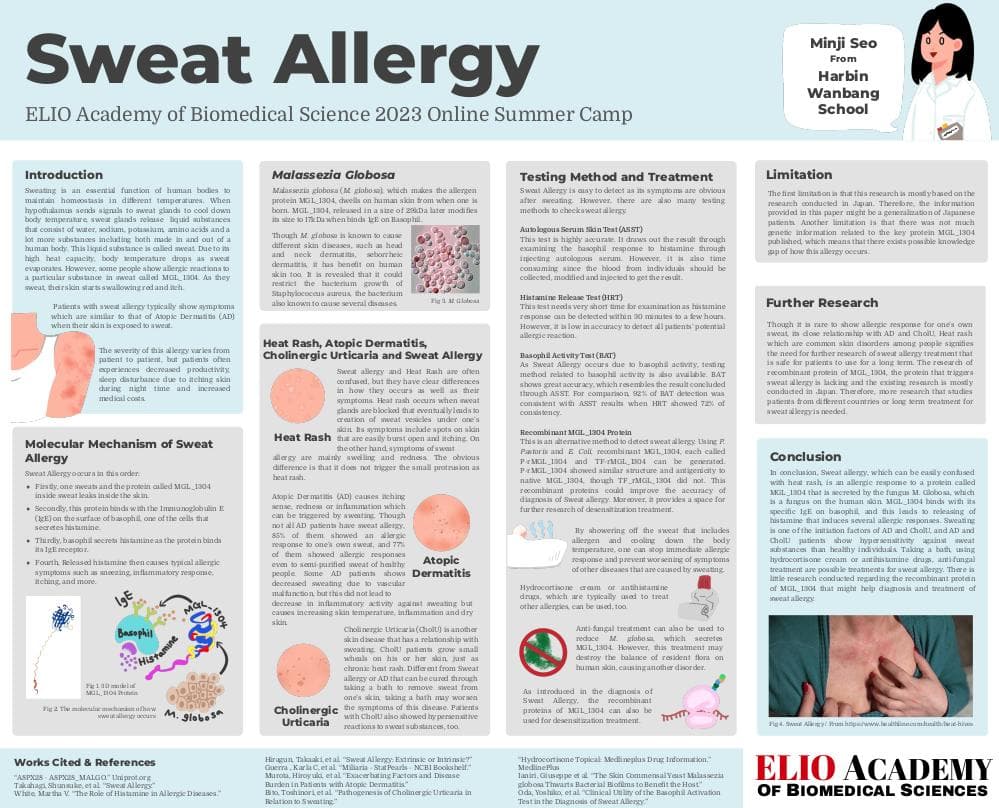
_Fig1. The skin of sweat allergy patient when exposed to sweat_ [Source](https://doi.org/10.1016/j.alit.2018.07.002)
Patients with sweat allergy typically exhibit symptoms similar to those of Atopic Dermatitis (AD) when their skin comes into contact with sweat. The severity of the reaction varies, but common symptoms include redness, mild swelling, irritating itch, and a prickling sensation. Sweat allergy can affect individuals of all ages, disrupting their normal lives due to dermatological symptoms. Sweat allergy patients experience daily disturbances such as reduced productivity, sleep disruptions from nighttime itching, and increased medical costs. As a result, even mild reactions can lead to heightened stress and irritability among patients. Interestingly, while sweat allergy is rare, many individuals experience skin issues after sweating. This paper will delve into the occurrence of sweat allergy, its treatment, and related conditions that might be mistaken for sweat allergy.
Pathology of Sweat allergy

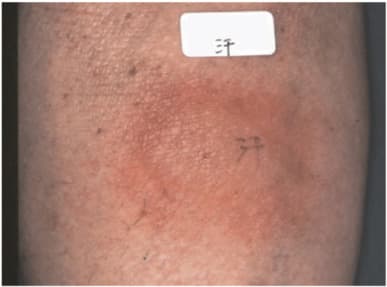
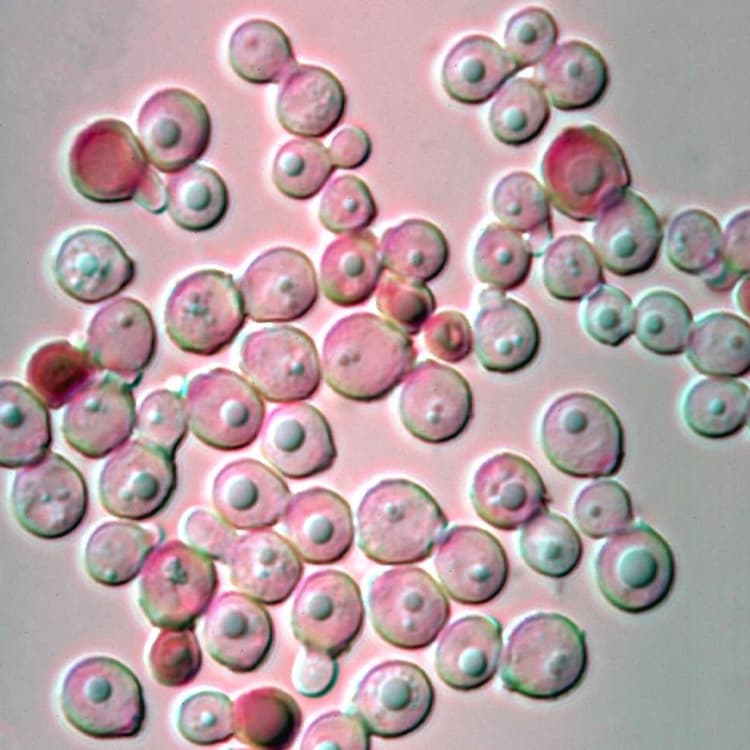
_Fig 2. 3D model of MGL_1304 Protein_ ([Source](https://www.uniprot.org/uniprotkb/A8PX28/entry))
Sweat allergy initiates when a specific substance in sweat binds with basophil, a cell responsible for releasing histamine. This allergenic substance is a protein named MGL_1304, produced by Malassezia globosa. Despite being an external protein, it can be identified in purified sweat. Histamine is released by basophils when the MGL_1304-specific IgE on their surface interacts with MGL_1304. Subsequently, the released histamine triggers conventional allergic manifestations, including sneezing, inflammatory reactions, itching, and more.

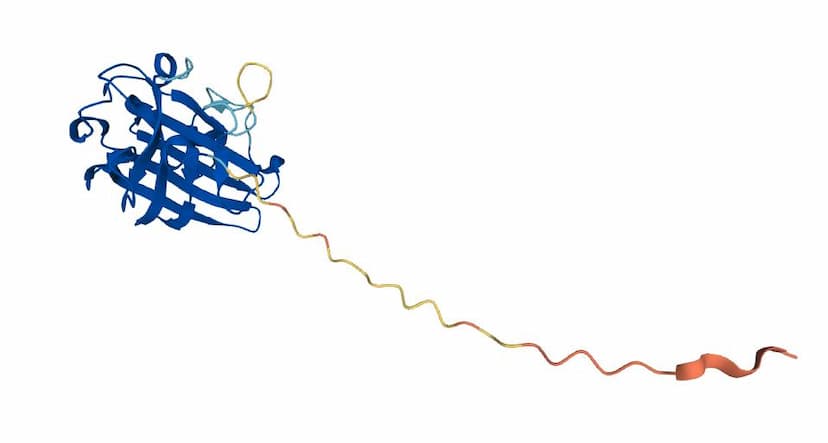
_Fig 3. Image of Malassezia globosa (M. Globosa)_ ([Source](https://commons.wikimedia.org/wiki/File:Malassezia_globosa_(14739397530).jpg))
Malassezia globosa (M. globosa), the producer of the allergenic protein MGL_1304, inhabits human skin from birth. This fungus is recognized for triggering various skin conditions like head and neck dermatitis, seborrheic dermatitis, and Malassezia folliculitis. When a patient perspires, the 29kDa-sized MGL_1304 protein undergoes a size modification to 17kDa. This altered protein subsequently binds with IgE, culminating in histamine release. Despite its role in different skin ailments, M. globosa also offers certain benefits to human skin. Giuseppe et al. discovered that M. globosa could inhibit the growth of Staphylococcus aureus bacteria, which is also associated with several diseases.
Difference between Sweat Allergy and Heat Rash
Sweat allergy and Heat Rash are frequently mistaken for each other due to their common triggers of sweating and resulting skin issues. Additionally, both conditions respond to cooling methods like bathing and avoiding further perspiration, contributing to the confusion or assumption that they are the same ailment. Nevertheless, Sweat allergy and Heat Rash exhibit distinct differences in mechanisms and symptoms.

_Fig 4. Model explaining the mechanism of Heat rash, it shows how sweat is re-flowing inside one's skin which makes a small vesicle under one's skin_ ([Source](https://www.mayoclinic.org/diseases-conditions/heat-rash/symptoms-causes/syc-20373276))
Heat Rash is not immunologically driven. It emerges when sweat glands become obstructed, leading to the development of sweat vesicles beneath the skin. Symptoms involve skin spots prone to bursting and accompanied by itching. Notably, the skin's small bumps resembling miniature water blisters are indicative of sweat accumulation beneath the surface.
Conversely, sweat allergy results from an immune system overreaction to a protein secreted by fungi residing on the skin. Consequently, its main symptoms encompass swelling and redness. The distinct contrast lies in the absence of the small bumps characteristic of heat rash.
Treatment
There are several treatments available for managing sweat allergy. The simplest approach involves taking a bath or shower, which helps remove sweat containing allergens and lowers body temperature, halting immediate allergic reactions. This method also prevents exacerbation of symptoms related to other sweat-induced conditions.
Another treatment option for sweat allergy is the use of hydrocortisone cream or antihistamine drugs, commonly employed to address allergic responses. However, these medications can have significant side effects on the patient's skin, including burning, itching, irritation, redness, dryness, acne, unwanted hair growth, and changes in skin color. Hence, cautious use of hydrocortisone cream or antihistamine drugs is necessary.
Anti-fungal treatment presents an alternative approach, given that the allergen originates from M. globosa, a type of fungi residing on human skin. Nonetheless, these treatments may disrupt the overall balance of skin-resident fungi, potentially leading to other disorders. As M. globosa plays a role in limiting the growth of S. aureus, various functions of fungal colonies on human skin have both positive and negative effects. Therefore, maintaining skin biome equilibrium is crucial throughout the treatment process.
Further Research
There is serious scarcity of research regarding the cause, mechanism, or genetic component regarding sweat allergy. Existing research mainly covers the sample groups consisting of Japanese. Therefore, research conducted in different countries should be conducted first for comparison and analysis between different groups of patients.
Testing Method

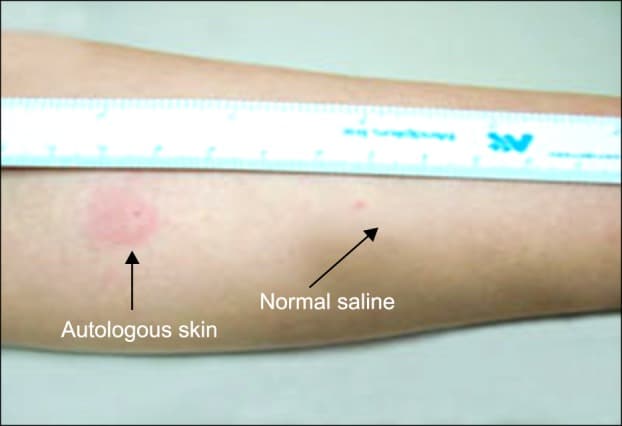
_Fig 5. The difference between normal saline testing and autologous skin test_ ([Source](https://www.researchgate.net/figure/Positive-results-of-Autologous-serum-skin-test-the-serum-injected-site-manifested-a_fig1_262811179))
Sweat allergy exhibits immediate reactions upon exposure to sweat and excessive heat on the skin, facilitating easy detection. Alternatively, various tests can be conducted to confirm its presence. One such test is the Autologous Serum Skin Test (ASST), which accurately assesses basophil response by injecting autologous serum. However, ASST is time-consuming due to the collection, modification, and injection of individual blood samples.
The Histamine Release Test (HRT) offers quicker results, detecting histamine responses within 30 minutes to a few hours. Nonetheless, its accuracy in identifying all potential allergic reactions is limited. Impaired IgE signaling or low histamine contents in basophils lead to non-responding basophils, decreasing the accuracy of HRT.
A more recent testing method, the Basophil Activity Test (BAT), evaluates basophil activity associated with sweat allergy. As sweat allergy is mainly associated with basophil activities, BAT demonstrates high accuracy similar to ASST results, with 92% consistency compared to HRT's 72%. BAT and HRT exhibit sensitivities of 100% and 44%, respectively. While BAT slightly lags in positive prediction accuracy (91.3% vs. 100%), it excels in negative prediction accuracy (100% vs. 30%) when compared to HRT.
Recent research by Takanobu et al. aims to develop an alternative detection method for sweat allergy. By employing P. Pastoris and E. Coli, they generated recombinant MGL_1304, termed P-rMGL_1304 and TF-rMGL_1304. P-rMGL_1304 closely resembled native MGL_1304 in structure and antigenicity, whereas TF-rMGL_1304 did not. This discovery is anticipated to enhance diagnostic accuracy for sweat allergy and open avenues for desensitization treatments using recombinant proteins.
Relationship With Atopic Dermatitis and Cholinergic Urticaria

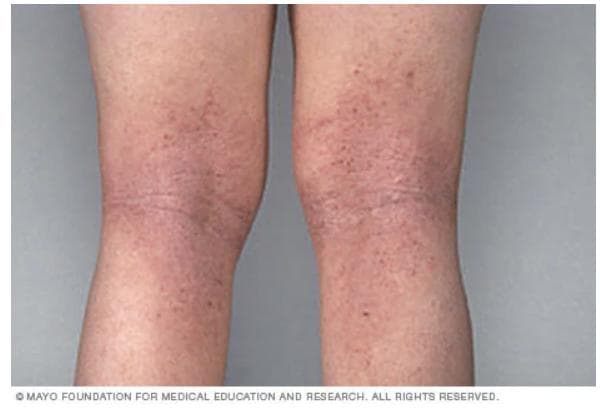
_Fig 6. Image of legs of Atopic Dermatitis patient_ ([Source](https://www.mayoclinic.org/diseases-conditions/atopic-dermatitis-eczema/symptoms-causes/syc-20353273))
While sweat allergy is rare, many individuals encounter diverse dermatological symptoms after sweating due to its association with various skin diseases. In addition to sweat allergy, sweating can trigger different skin conditions. As previously discussed, heat rash is one such condition. Notably, sweating is closely linked to Atopic Dermatitis (AD) and Cholinergic Urticaria. AD, characterized by skin inflammation, itching, and redness, often exhibits a familial predisposition. Sweating is recognized as an exacerbating factor for AD. While not all AD patients have sweat allergy, 85% display an allergic reaction to their own sweat, and 77% react allergically to semi-purified sweat from healthy individuals. This suggests that Basophils in AD patients exhibit heightened sensitivity to MGL_1304 in sweat from any source. Although hypersensitive IgE responses to sweat substances are a clear factor in the development of AD and sweat allergy, some AD patients experience reduced sweating due to vascular dysfunction. This condition doesn't decrease the inflammatory response to sweating but leads to elevated skin temperature, inflammation, and dry skin, exacerbating their skin condition.


_Fig 7. The wheals of Cholinergic Urticaria on patient's skin_ ([Source](https://dermnetnz.org/images/cholinergic-urticaria-images))
Cholinergic Urticaria (CholU) is another skin condition linked to sweating. CholU patients develop small wheals on their skin, resembling chronic heat rash. Unlike Sweat allergy or AD, which can be alleviated by bathing to remove sweat, bathing may exacerbate CholU symptoms. Patients with CholU exhibit hypersensitive reactions to sweat substances from both healthy individuals and fellow patients. Notably, CholU patients with sweat hypersensitivity are categorized as one group within various CholU subtypes. The research demonstrating the potential of using antigen desensitization present in sweat to treat CholU symptoms offers further support for the strong relationship between CholU and sweat allergy.
Conclusion
In conclusion, Sweat allergy, often mistaken for heat rash, is an allergic response to the protein MGL_1304 secreted by the fungus M. Globosa present on human skin. MGL_1304 binds with its specific IgE on basophils, triggering histamine release and inducing allergic reactions. Sweating serves as an initiating factor for conditions like AD and CholU, where patients exhibit heightened sensitivity to sweat substances. Treatments for sweat allergy include bathing, hydrocortisone cream, antihistamine drugs, and anti-fungal approaches. Limited research on the recombinant MGL_1304 protein for diagnosis and treatment suggests the need for further investigation, especially outside Japan. Given the link to chronic skin disorders like AD and CholU, patient safety in long-term treatment is essential.
Further Direction of Research
While allergic responses to one's own sweat are rare, the strong associations with AD, CholU, and Heat rash underscore the necessity for safe, long-term sweat allergy treatments. Research on the recombinant MGL_1304 protein is limited, primarily conducted in Japan. Therefore, extended studies involving patients from diverse countries or investigating the long-term treatment of sweat allergy are crucial. As sweat allergy correlates with chronic skin disorders such as AD and CholU, treatment safety should be a priority.
Limitation
Most research on sweat allergy specifically originates from Japan, potentially generalizing findings to Japanese patients and overlooking possible cross-country differences. Additionally, there is limited published genetic information about the key protein MGL_1304, further constraining this research. Therefore, in-depth investigations into the molecular mechanisms of sweat allergy, its connections with other skin disorders (AD or CholU), and treatment options are imperative to offer a more precise understanding of sweat allergy.


Impact Statement
I am Minji Seo from Harbin Wanbang school. I am studying abroad in Harbin, China, as a Korean student, enjoying my senior year. The topic of my project was inspired from my daily experience of my skin that always itches after sweating. I used to call it “sweat allergy,” but I wanted to research the biological mechanism and treatment of this dermatological disorder to accurately know what I am suffering from. Fortunately, I had a chance to conduct comprehensive research during the ELIO summer program, and this program led me to self-teach myself about the dermatological disorder triggered by sweating. ELIO academy offers a wonderful program that teaches the students how to dig deeper about a topic they are interested in. The information about biomedical science it teaches is of course wonderful, but I really appreciate the experience of interacting with Ms. Juhi and other students who are so passionate in the same field as me. I would recommend this program for anyone who is interested in biomedical science.
Student Reflection
Works Cited
"A8PX28 · A8PX28MALGO." _Uniprot, 22 Feb. 2023, www.uniprot.org/uniprotkb/A8PX28/entry.
"Allergy Skin Tests." Mayo Clinic, 6 Jan. 2022, www.mayoclinic.org/tests-procedures/allergy-tests/about/pac-20392895.
Bito, Toshinori, et al. "Pathogenesis of Cholinergic Urticaria in Relation to Sweating." Allergology International, vol. 61, no. 4, 29 July 2012, pp. 539–544, https://doi.org/10.2332/allergolint.12-rai-0485.
Ganguly, Satyaki, et al. "Autologous Serum Skin Test as an Indicator of Chronic Autoimmune Urticaria in a Tertiary Care Hospital in South India." Indian Dermatology Online Journal, vol. 5, no. 6, Dec. 2014, pp. 87–91, https://doi.org/10.4103/2229-5178.146166.
Ghosh, SudipKumar, and Sanjay Ghosh. "Autologous Serum Skin Test." Indian Journal of Dermatology, vol. 54, no. 1, winter 2009, pp. 86–87, https://doi.org/10.4103/0019-5154.49000.
Guerra , Karla C, et al. "Miliaria - StatPearls - NCBI Bookshelf." Miliaria, 28 Aug. 2022, www.ncbi.nlm.nih.gov/books/NBK537176/.
Hiragun, Takaaki, et al. "Sweat Allergy: Extrinsic or Intrinsic?" Journal of Dermatological Science, vol. 87, no. 1, 8 Mar. 2017, pp. 3–9, https://doi.org/10.1016/j.jdermsci.2017.03.002.
"Hydrocortisone Topical: Medlineplus Drug Information." MedlinePlus, 15 Jan. 2018, https://medlineplus.gov/druginfo/meds/a682793.html
Ianiri, Giuseppe, et al. "The Skin Commensal Yeast Malassezia Globosa Thwarts Bacterial Biofilms to Benefit the Host." Journal of Investigative Dermatology, vol. 138, no. 5, 21 Feb. 2020, pp. 1026–1029, https://doi.org/10.1016/j.jid.2018.01.008.
Kan, Takanobu, et al. "Evaluation of Recombinant MGL1304 Produced by Pichia Pastoris for Clinical Application to Sweat Allergy." _Allergology International, vol. 64, no. 3, 25 June 2015, pp. 266–271, https://doi.org/10.1016/j.alit.2015.03.003.
Murota, Hiroyuki, et al. "Exacerbating Factors and Disease Burden in Patients with Atopic Dermatitis." Allergology International, vol. 71, no. 1, Jan. 2022, pp. 25–30, https://doi.org/10.1016/j.alit.2021.10.002.
Oda, Yoshiko, et al. "Clinical Utility of the Basophil Activation Test in the Diagnosis of Sweat Allergy." Allergology International, vol. 69, no. 2, 30 Mar. 2020, pp. 261–267, https://doi.org/10.1016/j.alit.2019.09.003
Salah, Samir, et al. "Prevalence of Skin Reactions and Self-Reported Allergies in 5 Countries with Their Social Impact Measured through Quality of Life Impairment." International Journal of Environmental Research and Public Health, vol. 18, no. 9, 2021, p. 4501, https://doi.org/10.3390/ijerph18094501
Takahagi, Shunsuke, et al. "Sweat Allergy." Allergology International, vol. 67, no. 4, Oct. 2018, pp. 435–441, https://doi.org/10.1016/j.alit.2018.07.002
White, Martha V. "The Role of Histamine in Allergic Diseases." Journal of Allergy and Clinical Immunology, vol. 86, no. 4, Oct. 1990, pp. 599–605, https://doi.org/10.1016/s0091-6749(05)80223-480223-4>) .
Pineda, Fernando, et al. “Role of histamine release test for the evaluation of patients with immediate hypersensitivity reactions to clavulanic acid.” International Archives of Allergy and Immunology, vol. 168, no. 4, 20 Feb. 2016, pp. 233–240, https://doi.org/10.1159/000443274.
_By: MinJi Seo_
The opinions expressed here are the views of the writer and do not necessarily reflect the views and opinions of Elio Academy.