Rheumatic Heart Disease
Assessing RHD Susceptibility Among Varying Regions

By: Ryan Cortenbach, Coral Academy of Science Las Vegas
Introduction
Rheumatic Heart Disease (RHD) is a systemic immune condition initially caused by an untreated streptococcus pyogenes throat infection, which then could develop into Acute Rheumatic Fever (ARF) if the patient does not receive medication. One or more episodes of ARF can trigger an autoimmune reaction that leads to severe valvular heart damage by inflammation (especially in genetically susceptible individuals), more commonly known as RHD. When inflamed, the mitral and aortic valves' leaflets can become scarred or damaged, which leads to regurgitation or stenosis of a person's blood. Susceptibility to RHD is most common, but not limited to, adolescent patients (typically patients who are 5 - 14 years old). This heart disease has seen an increase in diagnosis, with over forty million confirmed cases to date, and more than 300,000 deaths every year. Despite this, research focused on preventing RHD is minimal and continues to present an extreme economic burden to various low and middle-income countries, with cases most pronounced in developing countries with inadequate healthcare, poor sanitary conditions, and overcrowded cities. Rheumatic Heart Disease is easily preventable through early diagnosis and treatment with prescription medicine like penicillin and amoxicillin.
Disease information
A person with Rheumatic Heart Disease (RHD) would first have to experience a pharyngeal Group A Streptococcus (GAS) infection and Acute Rheumatic Fever (ARF) symptoms to finally undergo signs of RHD. When a person feels symptoms like a sore throat, pain while swallowing, painful or tender joints, chills, vomiting, nausea, abdominal pain, or head and muscle aches, and they believe they have been in a GAS-prone environment, a trip to their local cardiologist is imperative. After examinations, a cardiologist may order a wide variety of screenings that scan your heart like echocardiograms, electrocardiograms, X-rays, cardiac MRIs, or blood tests.

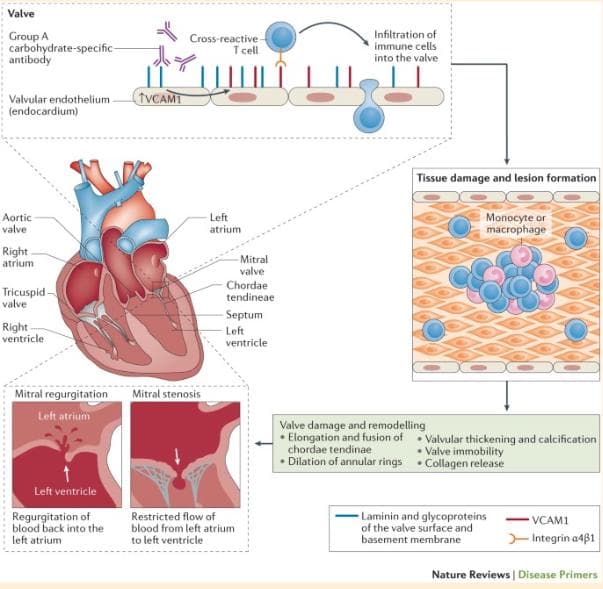
Demonstration of GAS pyogenes infecting the heart and causing regurgitation/stenosis (Source)
To diagnose RHD most accurately, echocardiographic screening combined with Doppler Echo ultrasonography or real-time 3-dimensional echo (RT3DE) is recommended. The Doppler Method excels in assessing Aortic Regurgitation and pressure gradients across aortic valves, while RT3DE is superior for identifying mitral valve malformations and the pathomechanism of Mitral Regurgitation (Saxena, 2013). For patients diagnosed with ARF, initial treatment involves anti-inflammatory medicine and salicylates to minimize inflammatory heart damage before considering prescription drugs like penicillin or amoxicillin to properly cure RHD damages (CDC, n.d.). Early detection and proper management of RHD are crucial for preventing severe cardiac complications.
Gene Level Information

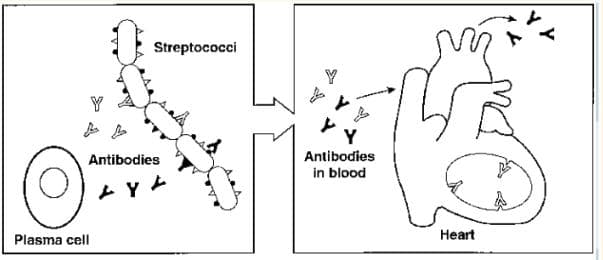
Plasma cells make antibodies against GAS antigens that cross-react, giving rise to inflammation. A demonstration of molecular mimicry. (Source)
Genome-wide association studies (GWAS) link RHD to the HLA-DQA1 to HLA-DQB1 region and the immunoglobulin heavy chain (IGH) locus, specifically the IGHV4-61 gene segment on chromosome 14. Genetic factors like HLA, cytokine, TGF-β, and MMP genes play a role. Gene involvement varies by region and ethnicity; an African-descending study identified genetic risk locus 11q24.1 (rs1219406) as a major contributor.
On-Going Research
Recent advancements in Rheumatic Heart Disease (RHD) prevention involve targeting socioeconomic determinants, household crowding, and dwelling characteristics that elevate infection risk. While vaccines against Group A Streptococcus (GAS), the RHD-causing bacterium, are in development, challenges persist due to bacterial genetic variations and limited commercial interest. Diagnostic methods for GAS pharyngitis have improved, using clinical decision rules and nucleic acid amplification tests. RHD treatment options span from medical management to valve surgery or repair, with explorations into transcatheter valve interventions. Global efforts to combat RHD are gaining momentum, marked by resolutions and calls for multisectoral collaboration to alleviate its global burden.

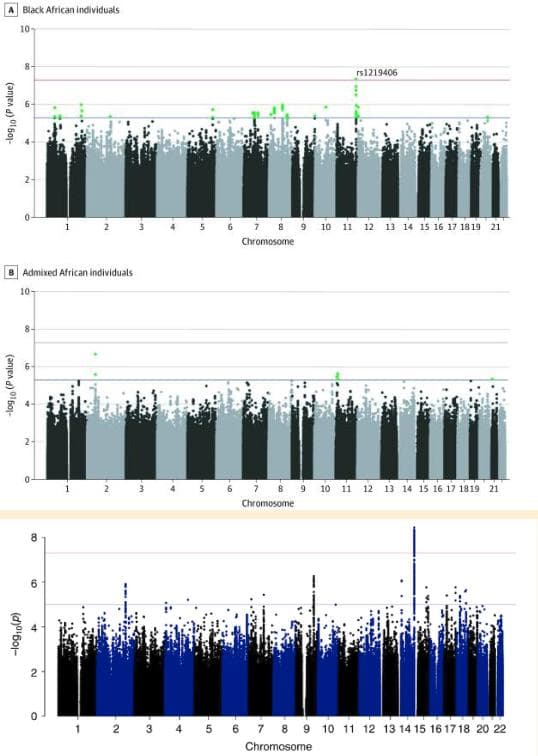
A Manhattan plot of the genetic susceptibility to Rheumatic Heart Disease that is exclusive to individuals living in the Oceania region. These two Manhattan plots demonstrate the genetic differences in susceptibility to Rheumatic Heart Disease in individuals depending on the regions they live in. (Source)
In the realm of proteomics, researchers utilized quantitative proteomics to identify a plasma protein signature of RHD in African patients. This signature, comprising six proteins (including adiponectin and complement component C7), effectively distinguished severe RHD cases from healthy controls. This suggests an ongoing inflammatory response during the chronic disease phase, potentially assisting in diagnosis and treatment. Lastly, researchers have uncovered novel connections in the expression of specific RNAs as a consequence of RHD. The study delved into the role of circulating exosomes and their contents, including long noncoding RNAs (lncRNAs) and messenger RNAs (mRNAs), in rheumatic heart disease (RHD). The study identified 231 differentially expressed lncRNAs and 179 mRNAs in the circulating exosomes of RHD patients compared to healthy controls. These distinct RNA patterns hold potential as diagnostic biomarkers for RHD. Particularly noteworthy, the study identified five pairs of co-regulated lncRNAs and their associated nearby genes, either upregulated or downregulated, in the circulating exosomes of RHD patients. These lncRNA-mRNA pairs could have significant implications for comprehending the molecular mechanisms underlying RHD development and progression.
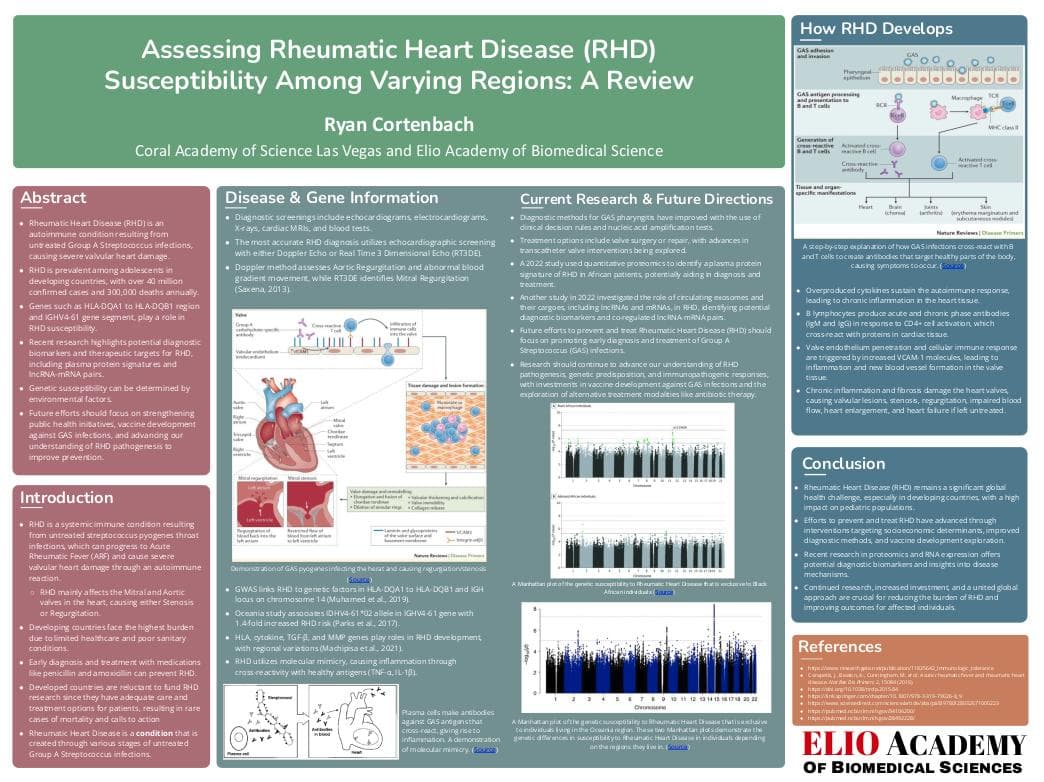
Immune Response against Streptococcus pyrogenes

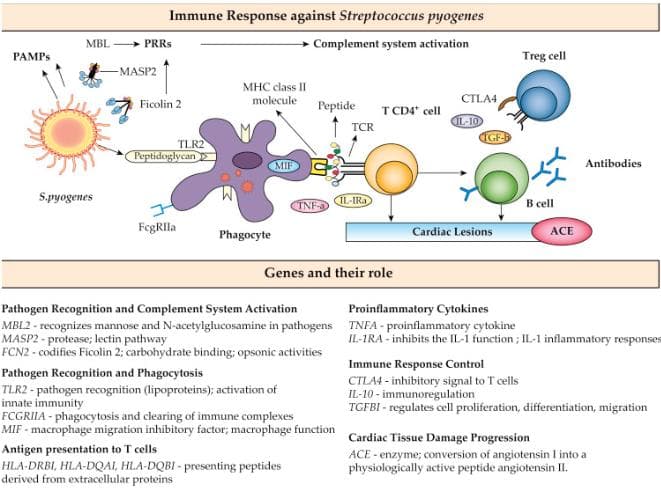
Rheumatic Heart Disease (RHD) arises as an autoimmune reaction due to untreated Group A Streptococcus (GAS) infections. It employs molecular mimicry, wherein GAS antigens activate T-cells that cross-react with heart tissue peptides, sparking inflammation. Excessive cytokines like TNF-alpha, IL-1, and IL-2 perpetuate the autoimmune response, leading to persistent heart tissue inflammation. Following GAS infection, B lymphocytes generate IgM and IgG antibodies in response to CD4+ cell activation, triggering antibody-T cell cross-reactivity with cardiac tissue proteins. Increased VCAM-1 levels result in CD4+ cell adherence and penetration into valve endothelium, initiating a valve-immune response. Inflammatory valve tissue, neovascularization, and antigenic expansion like vimentin and tropomyosin occur, broadening T-cell attacks. Subsequent to heart endocardial layer formation, white blood cell granulomas lead to inflammation and calcification. Individuals with RHD exhibit elevated osteopontin, CRP, and other inflammation markers. The prolonged immune reaction damages heart valves, inducing valvular lesions, stenosis, and regurgitation. Chronic inflammation and fibrosis impair heart function, causing reduced blood flow, heart enlargement, and failure. Untreated, RHD advances, posing severe complications and substantial cardiac risk. Timely diagnosis, GAS infection management, and RHD treatment are vital to hinder progression and mitigate heart impact.

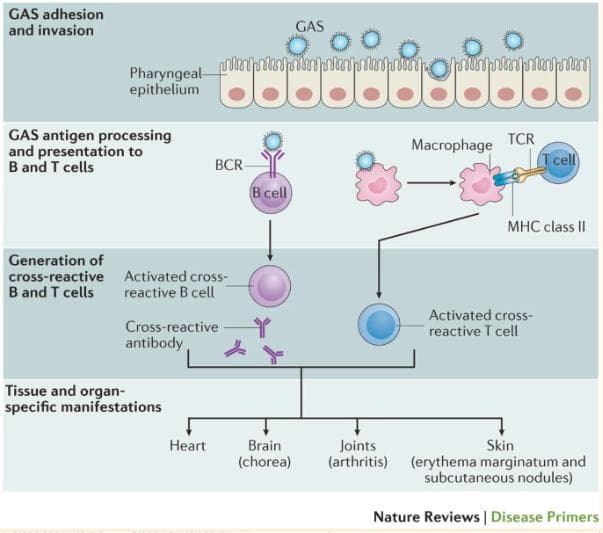
A step-by-step explanation of how GAS infections cross-react with B and T cells to create antibodies that target healthy parts of the body, causing symptoms to occur. (Source)
Future Directions/Treatment
To effectively prevent and treat Rheumatic Heart Disease (RHD), a comprehensive approach across various domains is imperative. Firstly, bolstering public health initiatives stands as a cornerstone in reducing the incidence of Group A Streptococcus (GAS) infections, a primary RHD trigger. Strengthening primary healthcare systems in resource-limited areas and promoting early detection and treatment of streptococcal infections can notably curtail RHD occurrences. Secondly, ongoing research should continue to deepen our comprehension of RHD pathogenesis and genetic susceptibility. In-depth investigations into molecular mimicry, collagen-associated neo-antigens, and T-cell receptor degeneracy can unveil novel therapeutic avenues. Furthermore, prioritizing the development of vaccines against GAS infections is crucial. Vaccination can significantly diminish the occurrence of streptococcal infections, subsequently thwarting the progression to RHD. Employing cutting-edge techniques such as single-cell RNA sequencing, researchers can gain profound insights into immunopathogenic responses, facilitating the creation of more efficacious treatment strategies. Alternatives like antibiotic therapy can also be considered in addition to vaccinations. Lastly, comprehending the impetigo route to RHD and delving deeper into how Rheumatic Heart Disease influences lncRNA and mRNA manipulation is pivotal. Recent research suggests that pharyngeal GAS infections might not be the sole path to developing acute rheumatic fever (ARF); skin infections are also implicated, challenging previous medical assumptions. Understanding RNA alterations is equally significant, as it can elucidate the cross-reactions and products driving cardiac inflammation, thereby enhancing RHD treatment approaches.
Conclusion
Rheumatic Heart Disease (RHD) remains a significant global health challenge, particularly in developing countries where it affects a substantial number of pediatric populations. Advances in preventing and treating RHD have been made, encompassing interventions targeting socioeconomic determinants, improved diagnostic methods, and the exploration of vaccine development. Nevertheless, the complexity of RHD and the necessity for multi-sectoral collaboration continue to present hurdles. Recent research in proteomics and RNA expression has unveiled new potential avenues for diagnostic biomarkers and insights into disease mechanisms. Moving forward, continuous research, heightened investment, and a united global approach are imperative to alleviate the burden of RHD and enhance outcomes for those impacted.


Impact Statement

Hello! I am Ryan Cortenbach, a Henderson, Nevada resident, proudly embracing my Ukrainian-Dutch heritage. I embarked on an academic journey exploring Rheumatic Heart Disease. This disease is endemic in developing nations, with more than 40 million cases reported worldwide and 300,000 fatalities yearly. Elio Academy's Genetics summer program became my guide in deciphering RHD's genetic intricacies. The program's mentorship offered tailored support, answering my every query with unwavering patience. Under my mentor's guidance, I navigated RHD's complexities with precision, and their expertise fortified my project. Armed with the newfound insights and tools from Elio Academy, I was able to decipher all the important data I needed to fully understand the genetic bounds of Rheumatic Heart Disease. Elio Academy harmonized learning and growth, encapsulating wisdom and camaraderie. With my fortified knowledge, I stride forth, contributing to the scientific dialogue on genetic maladies like RHD, profoundly impacted by Elio Academy.
Student Reflection
References
Abo, A., et al. (2022). Mechanistic insights into the pathophysiology of rheumatic heart disease. Clinical Proteomics, 19, 36. https://www.clinicalproteomicsjournal.biomedcentral.com/articles/10.1186/s12014-022-09345-1
Carapetis, J. R., et al. (2016). Acute rheumatic fever. Nature Reviews Disease Primers, 2, 15084. https://www.nature.com/articles/nrdp201584
Cooper, L. T. Jr., & El Accaoui, R. (2021). IL-6 as a new diagnostic biomarker for acute rheumatic carditis. Frontiers in Immunology, 12, 645232. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6956112/
El-Rachidi, R. M., et al. (2021). Echocardiographic predictors of left atrial spontaneous echo contrast and thrombi in patients with rheumatic heart disease. Frontiers in Cardiovascular Medicine, 8, 716716. https://www.frontiersin.org/articles/10.3389/fcvm.2021.716716/full
Eloi Marijon and others. (2021). Persisting burden and challenges of rheumatic heart disease. European Heart Journal, 42(34), 3338–3348. https://doi.org/10.1093/eurheartj/ehab407
European Heart Journal. (2021). Volume 42, Issue 34. https://academic.oup.com/eurheartj/issue/42/34
Hare, M. J., et al. (2008). Searching for molecular markers of rheumatic heart disease: do we need more information? Medical Journal of Australia, 189(10), 565-566. https://www.mja.com.au/journal/2008/189/10/searching-molecular-markers-rheumatic-heart-disease-do-we-really-need-more
How are group A streptococci spread? (n.d.). New York State Department of Health. https://www.health.ny.gov/diseases/communicable/streptococcal/group_a/fact_sheet.htm.
How does the heart work? (n.d.). News-Medical.Net. https://www.news-medical.net/health/Structure-and-Function-of-the-Heart.aspx
How does the human heart work? (n.d.). Hopkins Medicine. https://www.hopkinsmedicine.org/health/conditions-and-diseases/rheumatic-heart-disease
How to manage Group A streptococcal infection. (n.d.). Johns Hopkins Medicine. https://www.hopkinsmedicine.org/health/conditions-and-diseases/strep-throat.
Mayo Clinic Staff. (2021). Rheumatic heart disease. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/rheumatic-fever/symptoms-causes/syc-20354588
Molecular mimicry between human and GAS proteins triggers proinflammatory cardiac valve-reactive T cells. (n.d.). ResearchGate. https://www.researchgate.net/figure/Acute-rheumatic-heart-disease-is-the-best-example-of-molecular-mimicry-Plasma-cells-make_fig2_11825642/actions#reference
Muhamed, B., Parks, T., & Sliwa, K. (2019). Genetics of rheumatic fever and rheumatic heart disease. Nature Reviews Cardiology. doi:10.1038/s41569-019-0258-2
Naud, P., & Maguy, A. (2021). Rheumatic heart disease pathophysiology. News-Medical.Net. https://www.news-medical.net/health/Rheumatic-heart-disease-pathophysiology.aspx
Pasricha, M., & Sharma, G. K. (2021). Approach to the patient with rheumatic heart disease: current status and future perspective. Journal of Community Hospital Internal Medicine Perspectives, 11(3), 257-261. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8337213/
Ralph, A. P., et al. (2018). The 2020 Australian Guideline for prevention, diagnosis, and management of acute rheumatic fever and rheumatic heart disease. Medical Journal of Australia, 212(9), 458-464. https://www.mja.com.au/journal/2019/212/9/2020-australian-guideline-prevention-diagnosis-and-management-acute-rheumatic-fever
Rheumatic heart disease. (n.d.). World Heart Federation. https://world-heart-federation.org/what-we-do/rheumatic-heart-disease/.
Rheumatic heart disease. (n.d.). World Health Organization. https://www.who.int/news-room/fact-sheets/detail/rheumatic-heart-disease#
Rudd, A., et al. (2016). Acute rheumatic fever and rheumatic heart disease in Mongolia. Heart Asia, 8(1), 31-37. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5087043/
Sabri, A., et al. (2018). Assessment of left atrial function in rheumatic heart disease using 2D speckle tracking echocardiography. Heart Views, 19(3), 86-91. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6103861/
Saleh, R., et al. (2011). Inflammatory pathways in the early stages of myocardial ischemia. The Lancet, 378(9792), 1932-1943. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3104525/.
Stollerman, G. H. (2007). Rheumatic fever. The Lancet, 370(9602), 887-898. https://pubmed.ncbi.nlm.nih.gov/17607501/
Turakhia, M. P., et al. (2021). Atrial fibrillation in rheumatic heart disease: epidemiology, pathophysiology, and novel therapies. Circulation, 143(13), 1327-1341. https://www.ahajournals.org/doi/10.1161/CIRCULATIONA
By: Ryan Cortenbach
The opinions expressed here are the views of the writer and do not necessarily reflect the views and opinions of Elio Academy.