Triple Negative Breast Cancer: Precision Medicine
By: Sadhika Pendyala, The Quarry Lane School

Triple Negative Breast Cancer (TNBC) accounts for 10 to 15% of breast cancer cases, with one of the worst prognosis. Triple Negative Breast Cancer is unique because of its lack of HER2, estrogen, and progesterone receptors present in tumors. This limitation greatly reduces treatment options because conventional therapeutic strategies, such as hormone-based treatments and inhibitors, are inefficient and lack efficacy.
Epidemiology
Triple Negative Breast Cancer (TNBC) represents 10%–20% of invasive breast cancers and is commonly associated with people of African-American descent, deprivation status, younger age at diagnosis, more advanced disease stage, high mitotic indices, family history of breast cancer, and BRCA1 mutations. Women who experience TNBC have a risk of recurrence within 3 years of diagnosis, and mortality rates increase 5 years after diagnosis. Studies involving patients with TNBC to determine external and social factors (e.g., smoking, alcoholism, and contraceptive usage) do not provide strong insight into what may cause TNBC. The SEER (Surveillance, Epidemiology, and End Results) program tracked by the National Cancer Institute shows that African American (AA) women, Non-Hispanic, and Hispanic alike, have the highest incidence rates of TNBC at all stages of diagnosis compared to other ethnicities. AA women are 1.5 times more likely to be diagnosed with TNBC compared to Non-Hispanic White and White women. Additionally, AA women may present more aggressive phenotypes of TNBC due to socioeconomic determinants and other health factors. Some socioeconomic factors that may contribute to TNBC disparity are non-preference of participation in trials, the risk of diabetes, hypertension, and the probability of AA patients accessing under-resourced hospitals. Genetic factors in AA women include BRCA1, p53, and AURKA/AURKB mutations. Some studies suggest that Cancer Stem Cells (CSC) may be a potential cause of the aggressive phenotype of TNBC expressed in AA women. Important CSCs to note are genes associated with the Wnt signaling pathway (TNC, Cav1, FOX03A, WNT10B, HMGA2) and ALDH1+. Also, many studies support the notion that TNBC tumors may be linked to issues with metabolism (e.g., insulin resistance, hypertension, dyslipidemia). Studies have shown a significant correlation between menopausal status and breast cancer subtypes, with TNBC correlated with postmenopausal patients. However, for TNBC, menopausal status was not correlated with tumor size and nodal size of the tumor.
Heterogeneity in TNBC
Based on multi-omics analyses, researchers have discovered that within TNBC, there are numerous epigenomic and genomic differences that exist between its subtypes, specifically certain CNAs (copy number alterations), mutational patterns, activation of protein pathways, and epigenetic factors. These extensive genetic sequencing studies suggest that TNBC subtypes potentially originate from different cells. Triple Negative Breast Cancer (TNBC) is a heterogeneous disease, meaning it consists of different subtypes with distinct characteristics. The classification of TNBC subtypes is evolving, and researchers use various molecular profiling techniques to identify and understand these subtypes. Following are some of the commonly recognized TNBC subtypes:
1. Basal-Like 1 (BL1): Characteristics: High proliferation, cell cycle-related gene expression. Associated Features: BRCA1 mutations, DNA damage response.
2. Basal-Like 2 (BL2): Characteristics: Immune response-related gene expression. Associated Features: Enriched for immune cell infiltrates.
3. Immunomodulatory (IM): Characteristics: High immune cell and cytokine-related gene expression. Associated Features: Presence of immune-related genes.
4. Mesenchymal (M): Characteristics: Mesenchymal and signaling pathway-related gene expression. Associated Features: Activation of signaling pathways involved in epithelial-mesenchymal transition (EMT).
5. Luminal Androgen Receptor (LAR): Characteristics: Hormone receptor and androgen receptor expression. Associated Features: Enriched for hormone receptor-related genes.
The BL1 (basal-like 1) subtype tumors and bipotent luminal progenitor cells seem to be closely related to one another, aligning with previous BRCA mutated mouse models. The LAR subtype of TNBC was linked to L2 hormone-responsive cells, which correlates with its dependency on hormone signaling. The CNAs and mutations observed between the BL1 and M (mesenchymal) subtype of TNBC propose that the M subtype may arise from the BL1 subtype. All of this suggests that TNBC subtypes may potentially originate from changes between cell states or different cell origins.

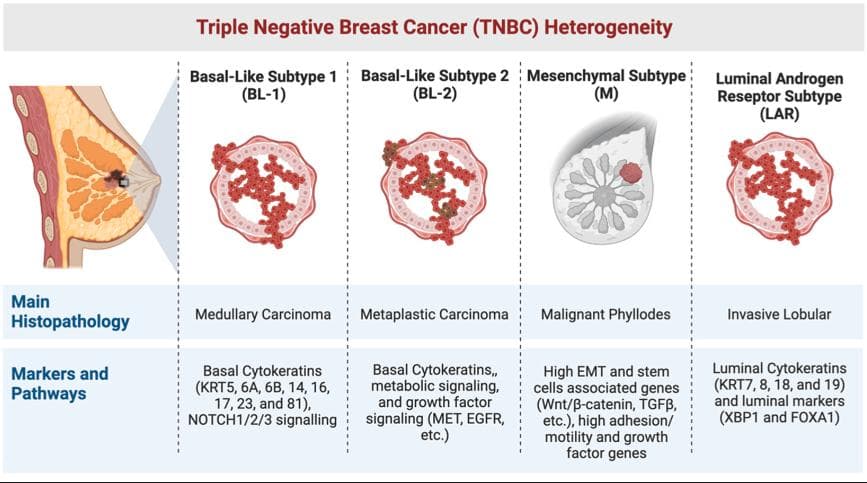
Figure. Table of heterogeneity that exists between different tumor subtypes in Triple Negative Breast Cancer. (Link)
Additionally, LAR subtypes and BL2 subtypes showed lower copy number alterations (CNAs) and mutations compared to other subtypes of TNBC. LAR subtype tumors demonstrated increased PI3K-AKT signaling and sensitivity to androgen receptor (AR) antagonist inhibitors. On the other hand, the BL2 subtypes were implicated in the MAPK pathway, and cell lines were observed to have increased sensitivity to MEK inhibitors. In comparison to the BL2 and LAR subtypes, the BL1 and M subtypes presented more mutational heterogeneity and issues with DNA homologous repair. These subtypes exhibited excessive amplification of MYC, a proto-oncogene, mutations in the NOTCH1/2/3 genes, and altered DNA repair protein expression. Although BL2 and M subtypes appeared to be sensitive to various inhibitors such as AURKA/B, PARP, and DNA-PK, it is unclear which is specifically implicated in tumorigenesis. The most viable therapeutic strategy would be to target the NOTCH pathway with γ-secretase inhibitors.
Etiology of TNBC
The etiology of Triple Negative Breast Cancer (TNBC) involves diverse factors, including genetic predisposition, hormonal influences, and molecular alterations. TNBC lacks estrogen, progesterone, and HER2 receptors, contributing to its aggressive nature. BRCA1 mutations and TP53 alterations are common genetic contributors. Younger age, African-American ethnicity, and specific socioeconomic factors correlate with increased risk. Hormonal signaling pathways, immune system dysregulation, and genomic instability further contribute to TNBC development. Understanding these multifaceted etiological aspects is crucial for targeted therapies and personalized interventions in combating this subtype of breast cancer.

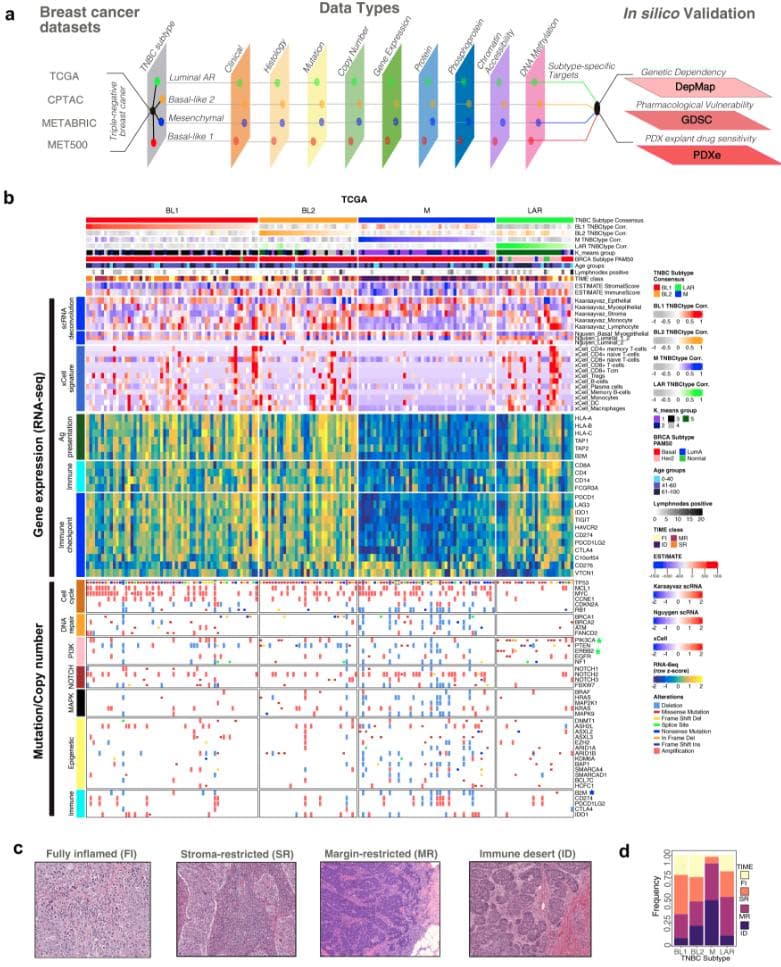
Figure. Multi-omics Analysis of the TNBC molecular subtypes presented as an oncoprint. (Link)
Biology and signaling Pathways underlying TNBC
Triple Negative Breast Cancer (TNBC) exhibits dysregulation in various signaling pathways, contributing to its aggressive nature. Key pathways involved include: PI3K-AKT-mTOR Pathway, MAPK/ERK Pathway, Notch Signaling, Wnt/β-Catenin Pathway, NF-κB Pathway, DNA Damage Response (DDR) Pathway. Understanding these signaling pathways provides insights into potential therapeutic targets for TNBC treatment. Targeted therapies aim to disrupt these pathways and inhibit cancer progression. Alternative strategies into identifying biomarkers include research into chemosensitive tumors to improve chances of patient survival while research into therapeutic targets is ongoing. Study at MD Anderson Research Center found that TNBC tumors that had mutations involved in the AR and FOXA1 pathway, which inhibits the PI3K/AKT pathway, were more sensitive to chemotherapy. Moreover, a lack of functional BRCA1/2 is associated with significantly improved patient outcomes. BRCA-deficient mutations have an increased rate of clonal mutations, associated with a greater immune response and effectively, a high chemosensitivity. Understanding the role of AR/FOXA1 in chemosensitive TNBC tumors provides insight into a novel marker and improves current chemotherapeutic regimens. This finding is essential as BRCA deficient subtypes compose 50% of the TNBC tumors that are immune primed. Other studies have looked into the DNA methylation biomarkers of TNBC, and found that ctDNA (circulating tumor DNA) provided invaluable knowledge about epigenetic and genetic factors.

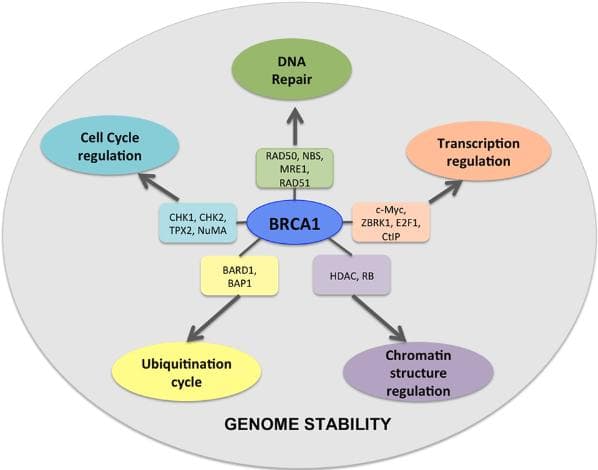
Figure. Diagram showing the ways in which BRCA1 influences other genetic factors to regulate different cellular processes and maintain genomic stability. (Link)
The promoter methylation of SFRP5, a component of the Wnt signaling pathway, was shown in 76.2% of breast tumor tissues, which is generally found unmethylated in regular breast tissue. The increased promoter methylation of SPHK2 was observed in BRCA-1 like breast tumors, in which a majority were TNBC. There is not a definitive group of genetic factors that impacts TNBC, as it is highly heterogeneous, and heavily influenced by its subtype tumor. Its mutational and unique genetic pattern vary patient to patient.


Figure. Mutations present in BRCA1 gene from CBioPortal Data, originally derived from breast cancer study at Memorial Sloan Kettering Cancer Center published in Nature. (Link)
BRCA regulation
Nearly 99% of TNBC subtype tumors consist of basal-like 1, and one of the key biomarkers associated with this is BRCA1. In triple-negative breast cancer (TNBC) cases, mutations in the BRCA1 and BRCA2 genes are identified. TNBC associated with these genetic mutations often exhibits distinct characteristics, displaying more aggressive behavior, an earlier onset, and a potential predisposition to bilateral breast cancer. The presence of BRCA1/2 mutations in TNBC has garnered considerable attention due to their role in DNA repair mechanisms. These mutations create vulnerabilities within cancer cells, making them potential targets for specialized therapies. While therapeutic approaches like PARP inhibitors have shown promise in targeting these vulnerabilities in BRCA-mutated cancers, their efficacy remains specifically relevant to this subset of TNBC cases. However, it's essential to acknowledge that a significant proportion of TNBC cases do not carry BRCA1/2 mutations. This diversity within TNBC implies that additional genetic and molecular factors contribute to its development. Understanding these alternate pathways beyond BRCA mutations is crucial for devising comprehensive treatment strategies that cater to the varied genetic landscapes observed in TNBC.
PI3K and AKT pathway
The PI3K/AKT pathway is a vital signaling cascade within cells that controls numerous cellular processes. It begins when extracellular signals, such as growth factors, bind to cell surface receptors, triggering the activation of phosphoinositide 3-kinase (PI3K). Activated PI3K modifies specific lipids in the cell membrane, generating phosphatidylinositol (3,4,5)-triphosphate (PIP3), a crucial signaling molecule. PIP3 serves as a docking site for AKT (also known as protein kinase B), recruiting it to the cell membrane through its pleckstrin homology (PH) domain. Once at the membrane, AKT undergoes a series of phosphorylation events, leading to its full activation. Activated AKT plays a central role in cell survival, growth, and metabolism by phosphorylating and regulating various downstream targets.

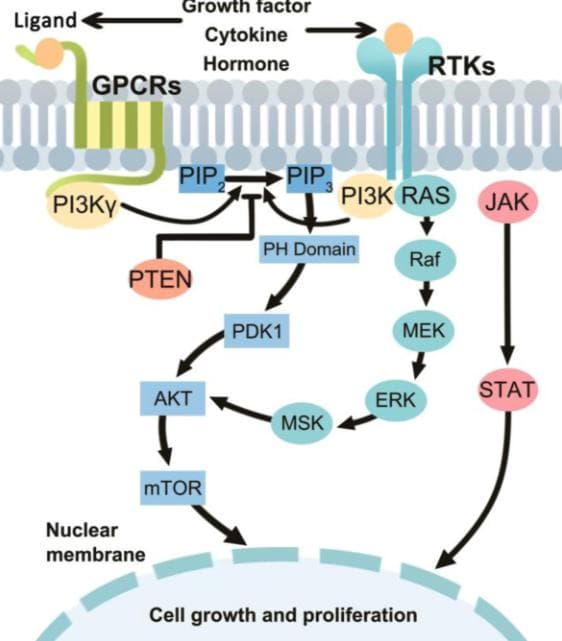
Figure. Illustration of the PI3K/AKT signaling pathway. (Link)
AKT's phosphorylation activity impacts proteins involved in cell cycle progression, protein synthesis, glucose metabolism, and cell survival pathways, thereby influencing the overall cell behavior.

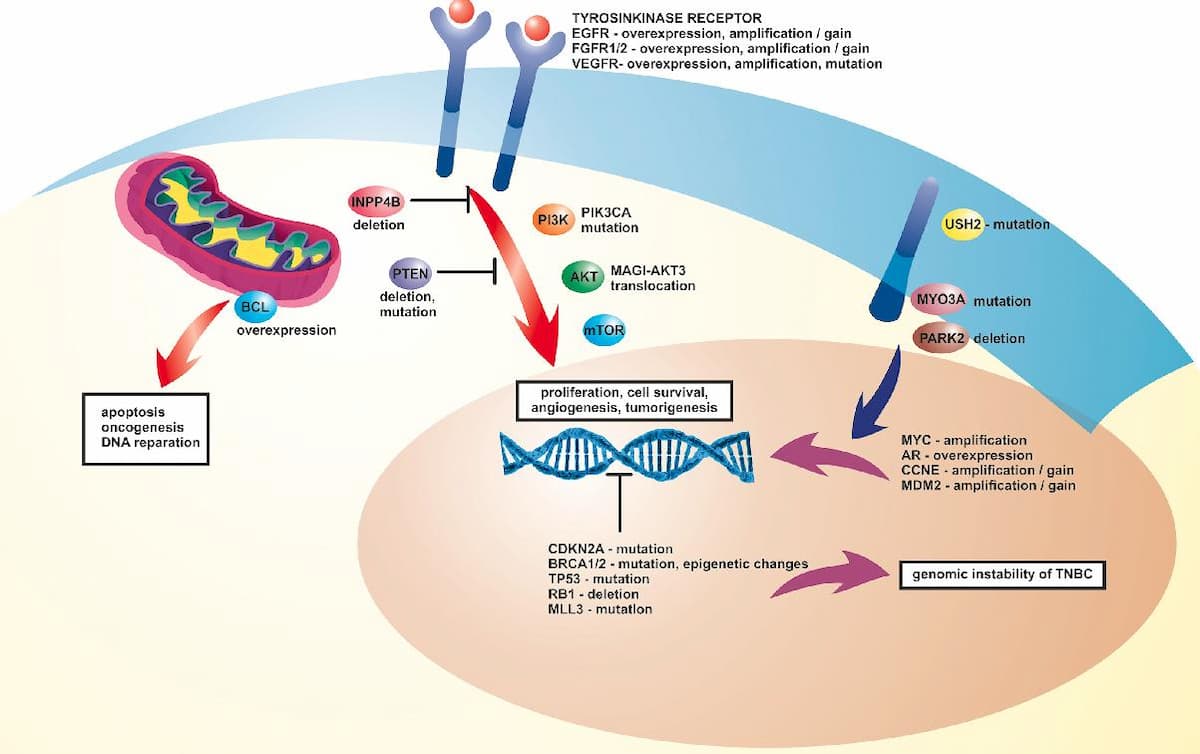
Figure. Diagram of the mutations and alternations of the PI3K/AKT pathway along with BRCA changes that create genomic instability of TNBC. (Link)
Dysregulation of the PI3K/AKT pathway is implicated in several diseases, including cancer, diabetes, and neurodegenerative disorders. It is vital to understand the role of PI3K/AKT pathway for this disease as it is implicated in the luminal androgen subtype (LAR) which is associated with the androgen/estrogen metabolism and steroid synthesis pathways. LAR subtypes showed sensitivity to PI3K inhibitors because of a mutation present in the PIK3CA, a gene that is responsible for the production of the key enzyme PI3K.

Figure. Mutations present in PIK3CA gene from CBioPortal Data, originally derived from breast cancer study at Memorial Sloan Kettering Cancer Center published in Nature. (Link)
Based on the same breast cancer study and CBioPortal discussed above, the most common alteration present in the PIK3CA mutation is H1047R gene with an amino acid change from leucine to tyrosine followed with E545K gene with an amino acid change from alanine to glutamine. Additionally, the PI3Ka domain showed the most frequent mutations. Exon 10 on Chromosome 3, where PIK3CA resides, contains the most mutations and protein changes which is also coupled with numerous instances of phosphorylation on residues. Nearly all of the mutations that exist for the PIK3CA gene are point mutations, specifically missense mutations which change the structure of the encoded protein. 78% of these mutations are somatic and the 138 mutations in PIK3CA collected from the patient sample are all point mutations.
Therapeutic Strategies
Chemotherapy
Chemotherapy plays a pivotal role in the management of Triple Negative Breast Cancer (TNBC), a subtype characterized by the absence of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) expression. TNBC is often more aggressive than other breast cancer subtypes, making chemotherapy a cornerstone of its treatment strategy. TNBC lacks specific targeted therapies, such as hormonal or HER2-directed therapies, making chemotherapy the primary systemic treatment option. The cytotoxic effects of chemotherapy aim to eradicate rapidly dividing cancer cells and reduce the risk of recurrence. Anthracyclines (e.g., doxorubicin) and taxanes (e.g., paclitaxel) are commonly used chemotherapy agents in TNBC. Neoadjuvant chemotherapy, administered before surgery, is frequently employed to shrink tumors and facilitate surgical resection. In some cases, a pathologic complete response (pCR) to neoadjuvant chemotherapy is associated with improved long-term outcomes. Adjuvant chemotherapy, given after surgery, aims to eliminate any remaining cancer cells and reduce the risk of recurrence. Given the aggressive nature of TNBC, chemotherapy regimens are often intensified, with combinations of different agents to maximize efficacy. Despite the success of chemotherapy in TNBC, challenges include potential toxicities and the need for more personalized treatment approaches. Ongoing research focuses on identifying predictive biomarkers and developing targeted therapies to enhance the effectiveness of chemotherapy while minimizing side effects.
PARP inhibitors
PARP inhibitors (Poly(ADP-ribose) polymerase inhibitors) have emerged as a promising class of targeted therapy for Triple Negative Breast Cancer (TNBC), a subtype known for its aggressive nature and lack of expression of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2). Understanding the molecular basis of TNBC is crucial for appreciating the role of PARP inhibitors in its treatment.TNBC is characterized by defects in DNA repair mechanisms, particularly in the homologous recombination pathway. PARP enzymes play a crucial role in DNA repair, and PARP inhibitors exploit this vulnerability in cancer cells. When PARP is inhibited, the cells with defective homologous recombination are unable to repair DNA damage effectively, leading to synthetic lethality. The most studied PARP inhibitors in TNBC include olaparib, talazoparib, and niraparib. Olaparib, the first FDA-approved PARP inhibitor, demonstrated efficacy in BRCA-mutated TNBC. BRCA1 and BRCA2 mutations are prevalent in TNBC, and olaparib's ability to exploit these deficiencies has shown significant clinical benefit. Talazoparib, another potent PARP inhibitor, has demonstrated superiority in terms of potency and efficacy in preclinical and clinical studies. Its ability to trap PARP on DNA leads to enhanced cytotoxicity. Niraparib, initially approved for ovarian cancer, has also shown promise in TNBC. It is being explored in clinical trials, and its effectiveness in homologous recombination-deficient cancers, including TNBC, is being investigated. The development of these PARP inhibitors represents a paradigm shift in the treatment of TNBC, providing a targeted approach for a subtype that lacks specific molecular targets. Despite their promise, challenges exist, such as identifying biomarkers beyond BRCA mutations to predict response and resistance mechanisms. Additionally, understanding the optimal combination strategies with chemotherapy or other targeted agents is essential for maximizing therapeutic outcomes. Ongoing research aims to elucidate these aspects, further refining the use of PARP inhibitors in TNBC treatment.
Checkpoint immunotherapy
Checkpoint immunotherapy for triple negative breast cancer (TNBC) involves drugs like pembrolizumab and atezolizumab blocking immune checkpoints, such as PD-1/PD-L1, to unleash the immune system against cancer cells. TNBC is characterized by higher PD-L1 expression, making it a potential target. Clinical trials are evaluating the efficacy of checkpoint inhibitors in TNBC, with some patients showing durable responses. However, not all patients benefit, and challenges like resistance exist. Combining checkpoint inhibitors with other treatments and identifying predictive biomarkers are areas of ongoing research to optimize immunotherapy outcomes for TNBC patients.
The disruption of DNA repair by PARP inhibitors can increase the tumor mutational burden, potentially making tumors more visible to the immune system, enhancing the efficacy of immunotherapies like immune checkpoint inhibitors. Targeting multiple pathways simultaneously by combining PARP inhibitors with targeted therapies has also gained attention. Combining olaparib with drugs targeting specific signaling pathways, such as PI3K or angiogenesis inhibitors, aims to exploit vulnerabilities in cancer cells and inhibit multiple survival pathways concurrently. Combining PARP inhibitors like olaparib with various classes of drugs, including chemotherapy, immunotherapy, targeted therapies, and inhibitors of DNA repair or cell cycle pathways, represents a multifaceted approach to enhance their therapeutic potential, overcome resistance, and improve outcomes for cancer patients.
Inhibitors targeting the PI3K/AKT pathway
Inhibitors targeting the PI3K/AKT Pathway have emerged as a promising therapeutic approach. Dysregulation of the PI3K/AKT pathway is frequently observed in TNBC, contributing to its aggressive nature and resistance to standard treatments. Inhibitors specifically targeting components of this pathway, such as PI3K inhibitors and AKT inhibitors, aim to disrupt the aberrant signaling cascade driving tumor growth and survival in TNBC. These inhibitors function by blocking key proteins involved in the pathway, thereby hindering tumor progression and potentially sensitizing TNBC cells to other treatments. Clinical trials exploring PI3K/AKT pathway inhibitors as monotherapies or in combination with standard chemotherapy or targeted therapies are underway. These trials aim to evaluate the efficacy and safety of these inhibitors in TNBC patients and identify optimal treatment strategies. Additionally, efforts are focused on understanding biomarkers or genetic signatures that could predict which TNBC patients are most likely to benefit from PI3K/AKT pathway inhibitors, aiding in personalized treatment approaches. While challenges like drug resistance and potential side effects persist, the development and utilization of these inhibitors represent a significant step toward targeted therapy for TNBC. The hope is that by precisely targeting the PI3K/AKT pathway, these inhibitors can offer new avenues for effective treatments, improving outcomes and quality of life for TNBC patients. Continued research and clinical investigations aim to refine the use of PI3K/AKT pathway inhibitors, potentially reshaping the landscape of TNBC therapy in the future.
Conclusion
In summary, Triple Negative Breast Cancer (TNBC) poses significant challenges due to its aggressive nature and limited treatment options. Disparities in incidence rates, molecular heterogeneity, and a lack of specific receptors complicate its management. Current strategies include intensified chemotherapy, PARP inhibitors targeting DNA repair deficiencies, and checkpoint immunotherapy leveraging the immune system. The identification of distinct TNBC subtypes, such as those associated with BRCA mutations or dysregulated PI3K/AKT pathways, opens avenues for personalized treatments. Ongoing research focuses on refining combination therapies and identifying biomarkers to enhance efficacy. While challenges persist, the multifaceted approach offers hope for improved outcomes in TNBC patients.


Impact Statement
Sadhika Pendyala
This project explored the biomarkers associated with triple negative breast cancer through an extensive understanding the epidemiology and the etiology. I also used cBioPortal to locate specific SNPs and post-translational modifications associated with this disease. The ERP program introduced me to various resources and tools that allowed me to expand my understanding of this topic. I learned about various statistical methods and bioinformatics techniques throughout this program and I greatly appreciated the guidance from my mentor for this project.
Student Reflection
Works Cited
Anders, C. K., Abramson, V., Tan, T., & Dent, R. (2016). The Evolution of Triple-Negative Breast Cancer: From Biology to Novel Therapeutics. American Society of Clinical Oncology Educational Book. American Society of Clinical Oncology. Annual Meeting, 35, 34–42. (https://doi.org/10.1200/EDBK_159135)
Bianchini, G., De Angelis, C., Licata, L., & Gianni, L. (2021). Treatment landscape of triple-negative breast cancer — expanded options, evolving needs. Nature Reviews Clinical Oncology, 19(2), 91–113. (https://doi.org/10.1038/s41571-021-00565-2)
Boyle, P. (2012). Triple-negative breast cancer: epidemiological considerations and recommendations. Annals of Oncology, 23(0923-7534), vi7–vi12. (https://doi.org/10.1093/annonc/mds187)
Jiang, T., Shi, W., Wali, V. B., Pongor, L. S., Li, C., Lau, R., Győrffy, B., Lifton, R. P., Symmans, W. F., Pusztai, L., & Hatzis, C. (2016). Predictors of Chemosensitivity in Triple Negative Breast Cancer: An Integrated Genomic Analysis. PLOS Medicine, 13(12), e1002193. (https://doi.org/10.1371/journal.pmed.1002193)
Lee, K.-L., Kuo, Y.-C., Ho, Y.-S., & Huang, Y.-H. (2019). Triple-Negative Breast Cancer: Current Understanding and Future Therapeutic Breakthrough Targeting Cancer Stemness. Cancers, 11(9), 1334. (https://doi.org/10.3390/cancers11091334)
Lehmann, B. D., Colaprico, A., Silva, T. C., Chen, J., An, H., Ban, Y., Huang, H., Wang, L., James, J. L., Balko, J. M., Gonzalez-Ericsson, P. I., Sanders, M. E., Zhang, B., Pietenpol, J. A., & Chen, X. S. (2021). Multi-omics analysis identifies therapeutic vulnerabilities in triple-negative breast cancer subtypes. Nature Communications, 12(1). (https://doi.org/10.1038/s41467-021-26502-6)
Lehmann, B. D., & Pietenpol, J. A. (2013). Identification and use of biomarkers in treatment strategies for triple-negative breast cancer subtypes. The Journal of Pathology, 232(2), 142–150. (https://doi.org/10.1002/path.4280)
Manoochehri, M., Borhani, N., Gerhäuser, C., Yassen Assenov, Maximilian Schönung, Hielscher, T., Christensen, B., Min Kyung Lee, Hermann-Josef Gröne, Lipka, D. B., Brüning, T., Brauch, H., Ko, Y.-D., & Hamann, U. (2022). DNA methylation biomarkers for noninvasive detection of triple‐negative breast cancer using liquid biopsy. International Journal of Cancer, 152(5), 1025–1035. (https://doi.org/10.1002/ijc.34337)
Mylavarapu, S., Das, A., & Roy, M. (2018). Role of BRCA Mutations in the Modulation of Response to Platinum Therapy. Frontiers in Oncology, 8(16). (https://doi.org/10.3389/fonc.2018.00016)
Ossovskaya, V., Wang, Y., Budoff, A., Xu, Q., Lituev, A., Potapova, O., Vansant, G., Monforte, J., & Daraselia, N. (2011). Exploring Molecular Pathways of Triple-Negative Breast Cancer. Genes & Cancer, 2(9), 870–879. (https://doi.org/10.1177/1947601911432496)
Razavi, P., Dickler, M. N., Shah, P. D., Toy, W., Brown, D. N., Won, H. H., Li, B. T., Shen, R., Vasan, N., Modi, S., Jhaveri, K., Caravella, B. A., Patil, S., Selenica, P., Zamora, S., Cowan, A. M., Comen, E., Singh, A., Covey, A., & Berger, M. F. (2020). Alterations in PTEN and ESR1 promote clinical resistance to alpelisib plus aromatase inhibitors. Nature Cancer, 1(4 ), 382–393. (https://doi.org/10.1038/s43018-020-0047-1)
Silva, J. (2020). Triple negative breast cancer: A thorough review of biomarkers. Critical Reviews in Oncology/Hematology, 145(1040-8428), 102855. (https://doi.org/10.1016/j.critrevonc.2019.102855)
Sporikova, Z., Koudelakova, V., Trojanec, R., & Hajduch, M. (2018). Genetic Markers in Triple-Negative Breast Cancer. Clinical Breast Cancer, 18(5), e841–e850. (https://doi.org/10.1016/j.clbc.2018.07.023)
Wang, D.-Y., Jiang, Z., Ben-David, Y., Woodgett, J. R., & Zacksenhaus, E. (2019). Molecular stratification within triple-negative breast cancer subtypes. Scientific Reports, 9(1), 19107. (https://doi.org/10.1038/s41598-019-55710-w)
Yang, J., Nie, J., Ma, X., Wei, Y., Peng, Y., & Wei, X. (2019). Targeting PI3K in cancer: mechanisms and advances in clinical trials. Molecular Cancer, 18(1). (https://doi.org/10.1186/s12943-019-0954-x)
Yin, L., Duan, J.-J., Bian, X.-W., & Yu, S. (2020). Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Research, 22(1). (https://doi.org/10.1186/s13058-020-01296-5)
Zagami, P., & Carey, L. A. (2022). Triple negative breast cancer: Pitfalls and progress. NPJ Breast Cancer, 8(1). (https://doi.org/10.1038/s41523-022-00468-0)
By: Sadhika Pendyala
The opinions expressed here are the views of the writer and do not necessarily reflect the views and opinions of Elio Academy.